Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
When performing a focused gastrointestinal system assessment, the practical nurse (PN) asks a male client when his last bowel movement occurred. The client answers, "Three days ago." Which action should the PN implement first?
A. Administer a prescribed PRN stool softener
Administering a stool softener without assessing the client's bowel patern may not be appropriate or effective
B. Determine the client's usual bowel patern
A bowel patern is the frequency, consistency, and appearance of a person's bowel movements. A normal bowel patern is what's normal for each person, and it can vary depending on factors such as diet, age, physical activity, and health conditions. A focused gastrointestinal system assessment includes collecting subjective data about the patient's history of gastrointestinal disease, signs and symptoms of gastrointestinal problems, diet and nutrition, and bowel patern. It also includes inspecting and auscultating the abdomen for any abnormalities. When a client reports having a bowel movement three days ago, the first action that the practical nurse should implement is to determine the client's usual bowel patern. This will help to evaluate if the client is experiencing constipation or if this is their normal frequency. It will also help to identify any changes or risk factors that may affect the client's bowel function.
C. Encourage the client to ambulate more frequently
Encouraging ambulation may help to stimulate bowel activity, but it is not the first action to take.
D. Recommend increasing high-fiber foods daily
Recommending dietary changes may be helpful for preventing or treating constipation, but it is not the first action to take.
This question is an excerpt from Nurse Dive's nursing test bank - HESI PN Exit 2023 Proctored Exam. Take the full exam now
Full Explanation
- A bowel patern is the frequency, consistency, and appearance of a person's bowel movements. A normal bowel patern is what's normal for each person, and it can vary depending on factors such as diet, age, physical activity, and health conditions.
- A focused gastrointestinal system assessment includes collecting subjective data about the patient's history of gastrointestinal disease, signs and symptoms of gastrointestinal problems, diet and nutrition, and bowel patern. It also includes inspecting and auscultating the abdomen for any abnormalities³.
- When a client reports having a bowel movement three days ago, the first action that the practical nurse should implement is to determine the client's usual bowel patern. This will help to evaluate if the client is experiencing constipation or if this is their normal frequency. It will also help to identify any changes or risk factors that may affect the client's bowel function.
Therefore, option B is the correct answer, while options A, C, and D are incorrect.
Option A is incorrect because administering a stool softener without assessing the client's bowel patern may not be appropriate or effective.
Option C is incorrect because encouraging ambulation may help to stimulate bowel activity, but it is not the first action to take.
Option D is incorrect because recommending dietary changes may be helpful for preventing or treating constipation, but it is not the first action to take.
Similar Questions
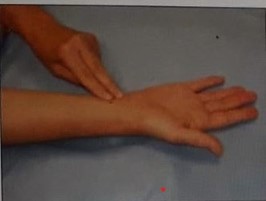
The practical nurse (PN) observes a newly hired unlicensed assistive personnel (UAP) who is counting a client's radial pulse as seen in the picture. Which action should the PN take?
A. Instruct the UAP to report any abnormal findings.
Instructing the UAP to report any abnormal findings does not address the error in technique.
B. Remind the UAP to check the client's pulse volume
Reminding the UAP to check the pulse volume does not address the error in technique.
C. Demonstrate the correct pulse site to the UAP
A radial pulse is the pulse felt at the wrist, where the radial artery runs along the thumb side of the forearm. It is one of the most common sites for measuring a person's heart rate. To measure a radial pulse, the examiner should place two or three fingers over the radial artery, just below the wrist crease, and apply gentle pressure until a pulsation is felt. The examiner should not use the thumb, as it has its own pulse and may interfere with the accuracy of the measurement. The examiner should count the number of beats for 15, 30, or 60 seconds, depending on the regularity and rate of the pulse. In the picture, the unlicensed assistive personnel (UAP) is using the thumb to measure the radial pulse, which is incorrect. The practical nurse (PN) should demonstrate the correct pulse site to the UAP and explain why using the thumb is not appropriate. This will help to ensure that the UAP obtains an accurate and reliable pulse rate for the client.
D. Confirm the accuracy of the pulse rate obtained by the UAP
Confirming the accuracy of the pulse rate obtained by the UAP does not address the error in technique.
Full Explanation
- A radial pulse is the pulse felt at the wrist, where the radial artery runs along the thumb side of the forearm. It is one of the most common sites for measuring a person's heart rate.
- To measure a radial pulse, the examiner should place two or three fingers over the radial artery, just below the wrist crease, and apply gentle pressure until a pulsation is felt. The examiner should not use the thumb, as it has its own pulse and may interfere with the accuracy of the measurement. The examiner should count the number of beats for 15, 30, or 60 seconds, depending on the regularity and rate of the pulse.
- In the picture, the unlicensed assistive personnel (UAP) is using the thumb to measure the radial pulse, which is incorrect. The practical nurse (PN) should demonstrate the correct pulse site to the UAP and explain why using the thumb is not appropriate. This will help to ensure that the UAP obtains an accurate and reliable pulse rate for the client.
Therefore, option C is the correct answer, while options A, B, and D are incorrect.
Option A is incorrect because instructing the UAP to report any abnormal findings does not address the error in technique.
Option B is incorrect because reminding the UAP to check the pulse volume does not address the error in technique.
Option D is incorrect because confirming the accuracy of the pulse rate obtained by the UAP does not address the error in technique.
When the practical nurse (PN) atempts to assist an 18-year-old client with a mild mental disability to ambulate on the first postoperative day after an appendectomy, she becomes angry and says, "PN, 'Get out of here! I'll get up when I'm ready!"
Which response is best for the PN to make?
A. A. "You must ambulate to avoid complications which could cause more discomfort than ambulating."
It uses a threatening tone and does not acknowledge the client's feelings.
B. B. "I know you feel angry about the pain of ambulation, but this is a necessary part of getting well."
It uses a threatening tone and does not acknowledge the client's feelings.
C. C. "Your healthcare provider has left specific instructions to ambulate on the first postoperative day."
It appeals to authority and does not explain the rationale or benefits of ambulation.
D. D. "I will be back in 30 minutes to help you get out of bed and walk around the room today."
An 18-year-old client with a mild mental disability is a client who has a lower than average intellectual functioning and some limitations in adaptive skills, such as communication, socialization, and self-care. A mild mental disability may affect the client's ability to understand, cope, or cooperate with medical interventions, such as ambulation after surgery. Ambulation is the act of walking or moving around. It is an important part of postoperative care, as it helps to prevent complications such as deep vein thrombosis, pulmonary embolism, pneumonia, atelectasis, constipation, and pressure ulcers. Ambulation also promotes circulation, wound healing, and muscle strength. When the practical nurse (PN) atempts to assist the client to ambulate on the first postoperative day after an appendectomy, the client becomes angry and says, "PN, 'Get out of here! I'll get up when I'm ready!" This may indicate that the client is experiencing pain, fear, anxiety, or frustration due to the surgery and the recovery process . The best response for the PN to make is to acknowledge the client's feelings, provide reassurance and support, and set a clear and realistic goal for ambulation. This will help to establish rapport, reduce resistance, and motivate the client to participate in the care plan. Therefore, option D is the correct answer, as it shows empathy and respect for the client's feelings, while also informing the client of the expectation and time frame for ambulation. Option D also allows the client some time to prepare mentally and physically for the activity.
Full Explanation
An 18-year-old client with a mild mental disability is a client who has a lower than average intellectual functioning and some limitations in adaptive skills, such as communication, socialization, and self-care. A mild mental disability may affect the client's ability to understand, cope, or cooperate with medical interventions, such as ambulation after surgery.
Ambulation is the act of walking or moving around. It is an important part of postoperative care, as it helps to prevent complications such as deep vein thrombosis, pulmonary embolism, pneumonia, atelectasis, constipation, and pressure ulcers. Ambulation also promotes circulation, wound healing, and muscle strength.
When the practical nurse (PN) atempts to assist the client to ambulate on the first postoperative day after an appendectomy, the client becomes angry and says, "PN, 'Get out of here! I'll get up when I'm ready!" This may indicate that the client is experiencing pain, fear, anxiety, or frustration due to the surgery and the recovery process .
The best response for the PN to make is to acknowledge the client's feelings, provide reassurance and support, and set a clear and realistic goal for ambulation. This will help to establish rapport, reduce resistance, and motivate the client to participate in the care plan.
Therefore, option D is the correct answer, as it shows empathy and respect for the client's feelings, while also informing the client of the expectation and time frame for ambulation. Option D also allows the client some time to prepare mentally and physically for the activity.
A client who received an open reduction and internal fixation (ORIF) of the right femur after experiencing a fall at home experiences a sudden onset of increasing confusion and agitation.
When reporting to the healthcare provider using SBAR (Situation, Background, Assessment, Recommendation) communication, which information should the nurse provide first?
A. Client's healthcare power of attorney.
Providing information about the client's healthcare power of attorney is not the most critical piece of information to report in this situation. The immediate concern is the client's change in mental status and potential medical emergency.
B. Fall at home as reason for admission.
While the reason for the client's admission is important background information, it is not the most urgent information to report in this situation. The priority is addressing the client's acute change in mental status.
C. Currently prescribed medications.
The nurse should be aware of the client's currently prescribed medications, but this information does not take precedence over the client's sudden onset of confusion and agitation. Immediate action is needed to address the client's altered mental status.
D. Increasing confusion of the client.
Increasing confusion and agitation in a client who recently underwent ORIF of the right femur is a significant change in condition and may indicate a medical emergency such as infection, delirium, or other complications. This information should be provided first to alert the healthcare provider to the client's immediate needs.
E. Increasing confusion of the client.
Full Explanation
Choice A rationale:
Providing information about the client's healthcare power of attorney is not the most critical piece of information to report in this situation. The immediate concern is the client's change in mental status and potential medical emergency.
Choice B rationale:
While the reason for the client's admission is important background information, it is not the most urgent information to report in this situation. The priority is addressing the client's acute change in mental status.
Choice C rationale:
The nurse should be aware of the client's currently prescribed medications, but this information does not take precedence over the client's sudden onset of confusion and agitation. Immediate action is needed to address the client's altered mental status.
Choice D rationale:
Increasing confusion and agitation in a client who recently underwent ORIF of the right femur is a significant change in condition and may indicate a medical emergency such as infection, delirium, or other complications. This information should be provided first to alert the healthcare provider to the client's immediate needs.