Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A 25-year-old gravida 2, para 2-0-0-2 gave birth 4 hours ago to a 9-lb, 7-ounce boy after augmentation of labor with Pitocin.
She puts on her call light and asks for her nurse right away, stating, “I’m bleeding a lot.” The most likely cause of afterbirth hemorrhage in this woman is:
A. Retained placental fragments.
This is when parts of the placenta remain attached to the uterine wall and prevent it from contracting properly. It is the second most common cause of postpartum hemorrhage. However, there is no indication in the question that the woman had any difficulty with the delivery of the placenta or that it was incomplete.
B. Unrepaired vaginal lacerations.
This is when there are tears or cuts in the vagina or cervix that cause bleeding. It is a less common cause of postpartum hemorrhage. However, there is no indication in the question that the woman had any trauma during delivery or that she was examined for lacerations.
C. Uterine atony
This is when the uterus does not contract enough to stop the bleeding from the placental site after delivery. It is the most common cause of postpartum hemorrhage, accounting for up to 80% of cases. Uterine atony can be caused by factors such as prolonged or augmented labor, large baby, multiple pregnancies, infection, or retained placenta. The woman in question has some risk factors for uterine atony, such as a large baby and augmentation of labor with Pitocin.
D. Puerperal infection
This is when there is an infection in the uterus or other parts of the reproductive tract after delivery. It can cause fever, pain, and bleeding. It is a rare cause of postpartum hemorrhage. However, there is no indication in the question that the woman had any signs or symptoms of infection, such as fever, chills, or foul-smelling discharge. Normal ranges for blood loss after delivery are less than 500 mL for vaginal birth and less than 1000 mL for C-section. Any amount above these thresholds can be considered postpartum hemorrhage and requires prompt evaluation and treatment.
This question is an excerpt from Nurse Dive's nursing test bank - OB Pediatric Cumulative Exam Test 4 V 1 2023 Proctored Exam. Take the full exam now
Full Explanation
Uterine atony.
This is when the uterus does not contract enough to stop the bleeding from the placental site after delivery. It is the most common cause of postpartum hemorrhage, accounting for up to 80% of cases. Uterine atony can be caused by factors such as prolonged or augmented labor, large baby, multiple pregnancies, infection, or retained placenta.
The woman in question has some risk factors for uterine atony, such as a large baby and augmentation of labor with Pitocin.
The other choices are wrong because:
A . Retained placental fragments: This is when parts of the placenta remain attached to the uterine wall and prevent it from contracting properly. It is the second most common cause of postpartum hemorrhage.
However, there is no indication in the question that the woman had any difficulty with the delivery of the placenta or that it was incomplete
B. Unrepaired vaginal lacerations: This is when there are tears or cuts in the vagina or cervix that cause bleeding. It is a less common cause of postpartum hemorrhage.
However, there is no indication in the question that the woman had any trauma during delivery or that she was examined for lacerations
D. Puerperal infection: This is when there is an infection in the uterus or other parts of the reproductive tract after delivery.
It can cause fever, pain, and bleeding. It is a rare cause of postpartum hemorrhage.
However, there is no indication in the question that the woman had any signs or symptoms of infection, such as fever, chills, or foul-smelling discharge.
Normal ranges for blood loss after delivery are less than 500 mL for vaginal birth and less than 1000 mL for C-section.
Any amount above these thresholds can be considered postpartum hemorrhage and requires prompt evaluation and treatment.
Similar Questions
What is an important nursing responsibility when dealing with a family experiencing the loss of an infant from sudden infant death syndrome (SIDS)?
A. Explain how SIDS could have been predicted and prevented.
Thisis wrong because explaining how SIDS could have been predicted and prevented is inappropriate. SIDS cannot be prevented or predicted. Discussions about the cause will only increase parental guilt.
B. Interview parents in-depth concerning the circumstances surrounding the infant’s death.
This is wrong because the parents should be asked only factual questions to determine the cause of death. Interviewing parents in-depth concerning the circumstances surrounding the infant’s death may be intrusive and stressful.
C. Discourage parents from making a last visit with the infant.
This is wrong because parents should be allowed and encouraged to make a last visit with their infant. Discouraging parents from making a last visit with the infant may deprive them of an opportunity to say goodbye and grieve.
D. Make a follow-up home visit to parents as soon as possible after the infant’s death.
Make a follow-up home visit to parents as soon as possible after the infant’s death. This is because a competent, qualified professional should visit the family at home as soon as possible after the death and provide the family with printed information about SIDS.
Full Explanation
choice D. Make a follow-up home visit to parents as soon as possible after the infant’s death. This is because a competent, qualified professional should visit the family at home as soon as possible after the death and provide the family with printed information about SIDS.
Choice A is wrong because explaining how SIDS could have been predicted and prevented is inappropriate.
SIDS cannot be prevented or predicted. Discussions about the cause will only increase parental guilt.
Choice B is wrong because the parents should be asked only factual questions to determine the cause of death. Interviewing parents in-depth concerning the circumstances surrounding the infant’s death may be intrusive and stressful.
Choice C is wrong because parents should be allowed and encouraged to make a last visit with their infant. Discouraging parents from making a last visit with the infant may deprive them of an opportunity to say goodbye and grieve.
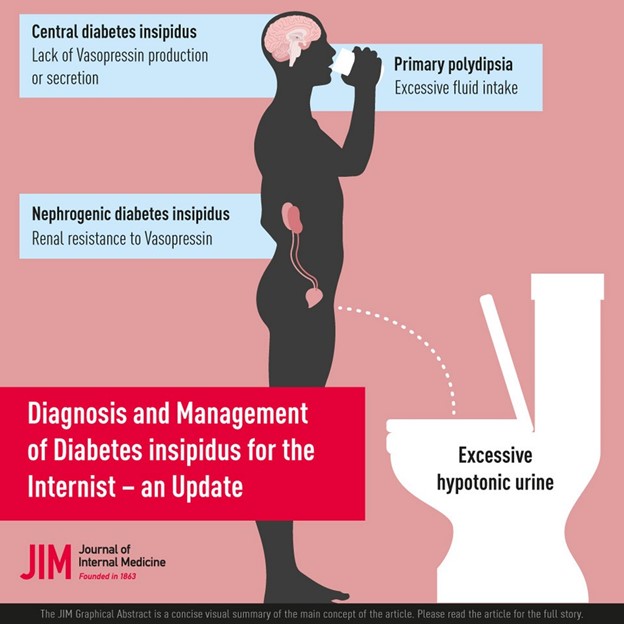
The nurse is caring for a child with suspected diabetes insipidus. Which clinical manifestation would be observable?
A. Oliguria
This is wrong because oliguria means decreased urine production and is not associated with diabetes insipidus.
B. Glycosuria
This is wrong because glycosuria means glucose in the urine and is associated with diabetes mellitus, not diabetes insipidus.
C. Nausea and vomiting
This is wrong because nausea and vomiting are associated with inappropriate ADH secretion (SIADH), which causes fluid retention and hyponatremia, not diabetes insipidus.
D. Polydipsia
Diabetes insipidus is a disorder of the posterior pituitary gland that causes a deficiency of antidiuretic hormone (ADH). This leads to excessive urination (polyuria) and excessive thirst (polydipsia) as the body tries to balance the fluid loss. These symptoms may be so severe that the child does little other than drink and urinate.
Full Explanation
Diabetes insipidus is a disorder of the posterior pituitary gland that causes a deficiency of antidiuretic hormone (ADH). This leads to excessive urination (polyuria) and excessive thirst (polydipsia) as the body tries to balance the fluid loss. These symptoms may be so severe that the child does little other than drink and urinate.
Choice A is wrong because oliguria means decreased urine production and is not associated with diabetes insipidus.
Choice B is wrong because glycosuria means glucose in the urine and is associated with diabetes mellitus, not diabetes insipidus.
Choice C is wrong because nausea and vomiting are associated with inappropriate ADH secretion (SIADH), which causes fluid retention and hyponatremia, not diabetes insipidus.
Cystic fibrosis (CF) is suspected in a toddler. Which test is essential in establishing this diagnosis?
A. Bronchoscopy
Thisis wrong because bronchoscopy is a procedure that allows the doctor to examine the airways and lungs, but it is not essential for diagnosing CF.
B. Serum calcium
This is wrong because serum calcium is a blood test that measures the level of calcium in the blood, which is not related to CF.
C. Urine creatinine
This is wrong because urine creatinine is a test that measures the amount of creatinine in the urine, which reflects the kidney function, but it is not relevant to CF. Normal ranges for sweat chloride test are: • Less than 40 millimoles per liter (mmol/L) for children and adults • Less than 30 mmol/L for infants younger than 6 months A sweat chloride level of more than 60 mmol/L is considered positive for CF.
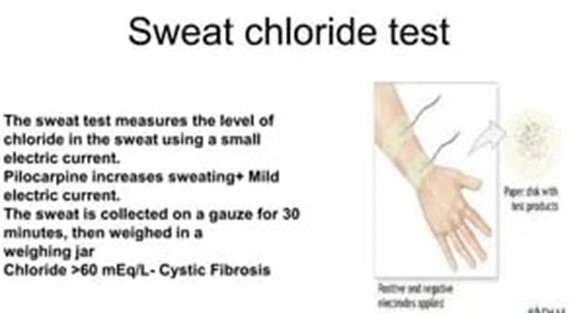
D. Sweat chloride test
This test measures the amount of chloride in the sweat, which is abnormally high in people with cystic fibrosis (CF). CF is an inherited disorder that affects the cells that produce mucus, sweat, and digestive juices.
Full Explanation
This test measures the amount of chloride in the sweat, which is abnormally high in people with cystic fibrosis (CF). CF is an inherited disorder that affects the cells that produce mucus, sweat, and digestive juices.
Choice A is wrong because bronchoscopy is a procedure that allows the doctor to examine the airways and lungs, but it is not essential for diagnosing CF.
Choice B is wrong because serum calcium is a blood test that measures the level of calcium in the blood, which is not related to CF.
Choice C is wrong because urine creatinine is a test that measures the amount of creatinine in the urine, which reflects the kidney function, but it is not relevant to CF.
Normal ranges for sweat chloride test are:
- Less than 40 millimoles per liter (mmol/L) for children and adults
- Less than 30 mmol/L for infants younger than 6 months
A sweat chloride level of more than 60 mmol/L is considered positive for CF.