Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A client is transported to the recovery area of the ambulatory care unit after cataract surgery. In which position does the nurse place the client?
A. Side lying on the affected eye.
Reason: Side lying on the affected eye is not the correct position for the client after cataract surgery, as it may increase intraocular pressure and cause bleeding or damage to the surgical site.
B. Supine
Reason: Supine is not the correct position for the client after cataract surgery, as it may cause fluid accumulation and swelling in the eye.
C. Prone
Reason: Prone is not the correct position for the client after cataract surgery, as it may cause pressure and friction on the eye.
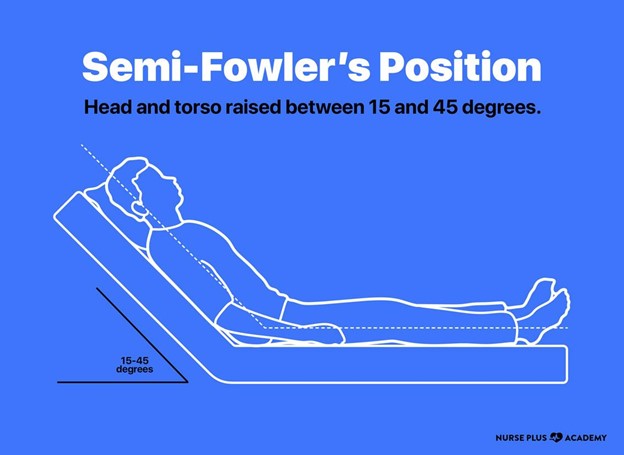
D. Semi Fowler's
Reason: Semi Fowler's is the correct position for the client after cataract surgery, as it helps to reduce intraocular pressure and promote drainage and healing of the eye.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Proctored Exam 3. Take the full exam now
Full Explanation
Choice A Reason: Side lying on the affected eye is not the correct position for the client after cataract surgery, as it may increase intraocular pressure and cause bleeding or damage to the surgical site.
Choice B Reason: Supine is not the correct position for the client after cataract surgery, as it may cause fluid accumulation and swelling in the eye.
Choice C Reason: Prone is not the correct position for the client after cataract surgery, as it may cause pressure and friction on the eye.
Choice D Reason: Semi Fowler's is the correct position for the client after cataract surgery, as it helps to reduce intraocular pressure and promote drainage and healing of the eye.
Similar Questions
A nurse in the ambulatory care unit is caring for a client after cataract extraction. The client suddenly complains of severe pain in the affected eye unrelieved by pain medications. Which of the following actions should the nurse take first?
A. Tell the client that this is to be expected after surgery.
Reason: Telling the client that this is to be expected after surgery is not the first action that the nurse should take, as it may indicate a complication such as increased intraocular pressure, hemorrhage, or infection.
B. Place the client in a supine position.
Reason: Placing the client in a supine position is not the first action that the nurse should take, as it may worsen the pain and increase intraocular pressure.
C. Document the findings.
Reason: Documenting the findings is not the first action that the nurse should take, as it may delay the intervention and outcome.
D. Notify the surgeon.
Reason: Notifying the surgeon is the first action that the nurse should take, as it indicates that the client needs immediate evaluation and treatment to prevent vision loss or permanent damage to the eye.
Full Explanation
Choice A Reason: Telling the client that this is to be expected after surgery is not the first action that the nurse should take, as it may indicate a complication such as increased intraocular pressure, hemorrhage, or infection.
Choice B Reason: Placing the client in a supine position is not the first action that the nurse should take, as it may worsen the pain and increase intraocular pressure.
Choice C Reason: Documenting the findings is not the first action that the nurse should take, as it may delay the intervention and outcome.
Choice D Reason: Notifying the surgeon is the first action that the nurse should take, as it indicates that the client needs immediate evaluation and treatment to prevent vision loss or permanent damage to the eye.
A nurse is planning to reinforce teaching with a client who has hemorrhoids. Which of the following information should the nurse plan to include in the instructions?
A. Follow a high-fiber diet to establish bowel regularity.
Reason: Following a high-fiber diet to establish bowel regularity is an appropriate instruction for a client who has hemorrhoids, as it helps to soften stools and reduce straining and pressure on hemorrhoids.
B. Use a stimulant laxative to prevent constipation.
Reason: Using a stimulant laxative to prevent constipation is not an appropriate instruction for a client who has hemorrhoids, as it may cause diarrhea, dehydration, or electrolyte imbalance.
C. Clean the anal area after bowel movements with alcohol-based wipes.
Reason: Cleaning the anal area after bowel movements with alcohol-based wipes is not an appropriate instruction for a client who has hemorrhoids, as it may irritate, dry, or damage hemorrhoidal tissue.
D. Limit the intake of fruit to prevent loose stools.
Reason: Limiting the intake of fruit to prevent loose stools is not an appropriate instruction for a client who has hemorrhoids, as fruit is a good source of fiber and fluid that can help prevent constipation and hemorrhoids.
Full Explanation
Choice A Reason: Following a high-fiber diet to establish bowel regularity is an appropriate instruction for a client who has hemorrhoids, as it helps to soften stools and reduce straining and pressure on hemorrhoids.
Choice B Reason: Using a stimulant laxative to prevent constipation is not an appropriate instruction for a client who has hemorrhoids, as it may cause diarrhea, dehydration, or electrolyte imbalance.
Choice C Reason: Cleaning the anal area after bowel movements with alcohol-based wipes is not an appropriate instruction for a client who has hemorrhoids, as it may irritate, dry, or damage hemorrhoidal tissue.
Choice D Reason: Limiting the intake of fruit to prevent loose stools is not an appropriate instruction for a client who has hemorrhoids, as fruit is a good source of fiber and fluid that can help prevent constipation and hemorrhoids.
A nurse is caring for a client who has type 1 diabetes mellitus. The nurse misread the client's morning blood glucose level as 310 mg/dL instead of 103 mg/dL and administered the insulin dose appropriate for a reading over 300 mg/dL. Which of the following actions should the nurse identify as the priority?
A. Call the RN supervisor.
Reason: Calling the RN supervisor is not the priority action for the nurse, as it may delay the intervention and outcome.
B. Complete an incident report.
Reason: Completing an incident report is not the priority action for the nurse, as it does not address the immediate problem or prevent further complications.
C. Check the blood glucose level.
Reason: Checking the blood glucose level is not the priority action for the nurse, as it may confirm the error but not correct it.
D. Give the client 15 to 20 g of carbohydrate.
Reason: Giving the client 15 to 20 g of carbohydrate is the priority action for the nurse, as it may prevent or treat hypoglycemia, which is a serious complication of insulin overdose.
Full Explanation
Choice A Reason: Calling the RN supervisor is not the priority action for the nurse, as it may delay the intervention and outcome.
Choice B Reason: Completing an incident report is not the priority action for the nurse, as it does not address the immediate problem or prevent further complications.
Choice C Reason: Checking the blood glucose level is not the priority action for the nurse, as it may confirm the error but not correct it.
Choice D Reason: Giving the client 15 to 20 g of carbohydrate is the priority action for the nurse, as it may prevent or treat hypoglycemia, which is a serious complication of insulin overdose.