Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is caring for a client who has type 1 diabetes mellitus. The nurse misread the client’s morning fasting blood glucose level as 210 mg/dL instead of 120 mg/dL and administered the insulin dose appropriate for reading over 200 mg/dL. Which of the following actions should the nurse identify as the priority?
A. Notify the nurse manager.
Choice A: Notify the nurse manager. This is an important action that the nurse should take, but not the priority. The nurse should notify the nurse manager to report the error and seek guidance on how to proceed. The nurse manager can also provide support and feedback to the nurse and help prevent similar errors in the future.
B. Give the client 15 to 20 g of carbohydrate.
Choice B: Give the client 15 to 20 g of carbohydrate. This is a necessary action that the nurse should take, but not the priority. The nurse should give the client 15 to 20 g of carbohydrate to raise their blood glucose level and prevent or treat hypoglycemia. The nurse should choose a fast-acting carbohydrate source, such as juice, glucose tablets, or candy.
C. Complete an incident report.
Choice C: Complete an incident report. This is a required action that the nurse should take, but not the priority. The nurse should complete an incident report to document the error and its consequences. The incident report can help identify the root cause of the error and improve patient safety and quality of care.
D. Check the client’s blood glucose level.
Choice D: Check the client’s blood glucose level. This is the priority action that the nurse should identify according to the ABCDE principle, which prioritizes interventions based on airway, breathing, circulation, disability, and exposure. The nurse should check the client’s blood glucose level to confirm the error and assess the risk of hypoglycemia, which is a low level of glucose in the blood. Hypoglycemia can cause symptoms such as sweating, trembling, confusion, and loss of consciousness. It can be life-threatening if not treated promptly.
This question is an excerpt from Nurse Dive's nursing test bank - ATI LPN Med Surg Proctored Exam. Take the full exam now
Full Explanation
Choice A: Notify the nurse manager. This is an important action that the nurse should take, but not a priority. The nurse should notify the nurse manager to report the error and seek guidance on how to proceed. The nurse manager can also provide support and feedback to the nurse and help prevent similar errors in the future.
Choice B: Give the client 15 to 20 g of carbohydrate. This is a necessary action that the nurse should take, but not the priority. The nurse should give the client 15 to 20 g of carbohydrates to raise their blood glucose level and prevent or treat hypoglycemia. The nurse should choose a fast-acting carbohydrate source, such as juice, glucose tablets, or candy.
Choice C: Complete an incident report. This is a required action that the nurse should take, but not the priority. The nurse should complete an incident report to document the error and its consequences. The incident report can help identify the root cause of the error and improve patient safety and quality of care.
Choice D: Check the client’s blood glucose level. This is the priority action that the nurse should identify according to the ABCDE principle, which prioritizes interventions based on airway, breathing, circulation, disability, and exposure. The nurse should check the client’s blood glucose level to confirm the error and assess the risk of hypoglycemia, which is a low level of glucose in the blood. Hypoglycemia can cause symptoms such as sweating, trembling, confusion, and loss of consciousness. It can be life-threatening if not treated promptly.
Similar Questions
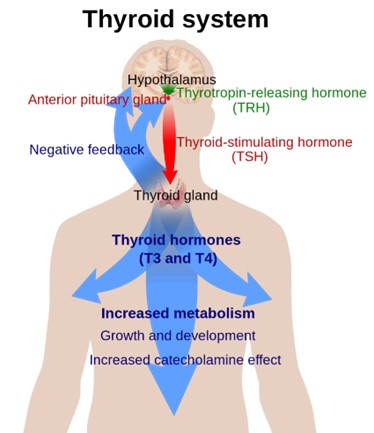
A nurse in a clinic is caring for a client who has a new diagnosis of hypothyroidism. Which of the following findings should the nurse expect?
A. Palpitations
Choice A: Palpitations. This is not a finding that the nurse should expect in a client who has a new diagnosis of hypothyroidism, but rather a sign of hyperthyroidism, which is a condition that occurs when the thyroid gland produces too much thyroid hormone. Hyperthyroidism can cause palpitations due to increased cardiac output and heart rate.
B. Weight gain
Choice B: Weight gain. This is a finding that the nurse should expect in a client who has a new diagnosis of hypothyroidism, which is a condition that occurs when the thyroid gland does not produce enough thyroid hormone. The thyroid hormone regulates the metabolism of carbohydrates, proteins, and fats, and affects energy expenditure and body temperature. Hypothyroidism can cause weight gain due to decreased metabolic rate and increased fluid retention.
C. Diaphoresis
Choice C: Diaphoresis. This is not a finding that the nurse should expect in a client who has a new diagnosis of hypothyroidism, but rather a sign of hyperthyroidism. Hyperthyroidism can cause diaphoresis due to increased heat production and vasodilation.
D. Protruding eyeballs
Choice D: Protruding eyeballs. This is not a finding that the nurse should expect in a client who has a new diagnosis of hypothyroidism, but rather a sign of Graves’ disease, which is an autoimmune disorder that causes hyperthyroidism. Graves’ disease can cause protruding eyeballs due to inflammation and edema of the orbital tissues and muscles.
Full Explanation
Choice A: Palpitations. This is not a finding that the nurse should expect in a client who has a new diagnosis of hypothyroidism, but rather a sign of hyperthyroidism, which is a condition that occurs when the thyroid gland produces too much thyroid hormone. Hyperthyroidism can cause palpitations due to increased cardiac output and heart rate.
Choice B: Weight gain. This is a finding that the nurse should expect in a client who has a new diagnosis of hypothyroidism, which is a condition that occurs when the thyroid gland does not produce enough thyroid hormone. The thyroid hormone regulates the metabolism of carbohydrates, proteins, and fats, and affects energy expenditure and body temperature. Hypothyroidism can cause weight gain due to decreased metabolic rate and increased fluid retention.
Choice C: Diaphoresis. This is not a finding that the nurse should expect in a client who has a new diagnosis of hypothyroidism, but rather a sign of hyperthyroidism. Hyperthyroidism can cause diaphoresis due to increased heat production and vasodilation.
Choice D: Protruding eyeballs. This is not a finding that the nurse should expect in a client who has a new diagnosis of hypothyroidism, but rather a sign of Graves’ disease, which is an autoimmune disorder that causes hyperthyroidism. Graves’ disease can cause protruding eyeballs due to inflammation and edema of the orbital tissues and muscles.
The nurse is caring for a client who has a bowel obstruction and a new prescription for the insertion of a nasogastric tube. Which of the following interventions should the nurse take when inserting the nasogastric tube?
A. Measure the tube for insertion from the tip of the nose to the umbilicus.
Choice A: Measure the tube for insertion from the tip of the nose to the umbilicus. This is not an intervention that the nurse should take when inserting a nasogastric tube. The nurse should measure the tube for insertion from the tip of the nose to the earlobe and then to the xiphoid process, which is a more accurate way of estimating the length of the tube needed to reach the stomach.
B. Place the client in a supine position.
Choice B: Place the client in a supine position. This is not an intervention that the nurse should take when inserting a nasogastric tube. The nurse should place the client in a high-Fowler’s position, which is a position with the head of the bed elevated to 90 degrees. This position can prevent aspiration, promote breathing, and allow gravity to assist with the insertion of the tube.
C. Withdraw the tube if the client gags during insertion.
Choice C: Withdraw the tube if the client gags during insertion. This is not an intervention that the nurse should take when inserting a nasogastric tube. The nurse should not withdraw the tube if the client gags during insertion, as this can cause trauma to the nasal or pharyngeal mucosa and increase discomfort. The nurse should pause and allow the client to rest and breathe until gagging subsides, then resume insertion. The nurse should also provide reassurance and encouragement to the client throughout the procedure.
D. Instruct the client to place his chin to his chest and swallow.
Choice D: Instruct the client to place his chin to his chest and swallow. This is an intervention that the nurse should take when inserting a nasogastric tube, which is a flexible tube that is inserted through the nose and into the stomach. The nurse should instruct the client to place his chin to his chest and swallow as the tube passes through the pharynx and into the esophagus. This can facilitate the insertion of the tube and prevent it from entering the trachea or causing injury to the nasal or pharyngeal mucosa.
Full Explanation
Choice A: Measure the tube for insertion from the tip of the nose to the umbilicus. This is not an intervention that the nurse should take when inserting a nasogastric tube. The nurse should measure the tube for insertion from the tip of the nose to the earlobe and then to the xiphoid process, which is a more accurate way of estimating the length of the tube needed to reach the stomach.
Choice B: Place the client in a supine position. This is not an intervention that the nurse should take when inserting a nasogastric tube. The nurse should place the client in a high-Fowler’s position, which is a position with the head of the bed elevated to 90 degrees. This position can prevent aspiration, promote breathing, and allow gravity to assist with the insertion of the tube.
Choice C: Withdraw the tube if the client gags during insertion. This is not an intervention that the nurse should take when inserting a nasogastric tube. The nurse should not withdraw the tube if the client gags during insertion, as this can cause trauma to the nasal or pharyngeal mucosa and increase discomfort. The nurse should pause and allow the client to rest and breathe until gagging subsides, then resume insertion. The nurse should also provide reassurance and encouragement to the client throughout the procedure.
Choice D: Instruct the client to place his chin to his chest and swallow. This is an intervention that the nurse should take when inserting a nasogastric tube, which is a flexible tube that is inserted through the nose and into the stomach. The nurse should instruct the client to place his chin to his chest and swallow as the tube passes through the pharynx and into the esophagus. This can facilitate the insertion of the tube and prevent it from entering the trachea or causing injury to the nasal or pharyngeal mucosa.
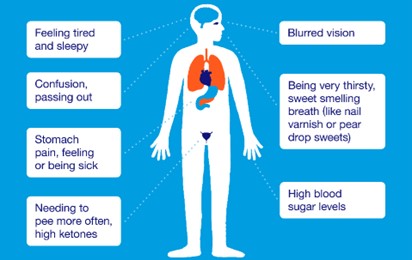
A nurse is collecting data from a client who has diabetes mellitus. Which of the following findings indicates that the client is experiencing DKA?
A. Rapid pulse
Choice A: Rapid pulse. This is not a finding that indicates that the client is experiencing DKA, but rather a sign of hypoglycemia, which is a low level of glucose in the blood. Hypoglycemia can cause rapid pulse due to increased sympathetic nervous system activity and decreased cardiac output.
B. Clammy skin
Choice B: Clammy skin. This is not a finding that indicates that the client is experiencing DKA, but rather a sign of hypoglycemia. Hypoglycemia can cause clammy skin due to increased sweating and vasoconstriction.
C. Confusion
Choice C: Confusion is commonly found in HHS rather than DKA.
D. Polydipsia
Choice D: Polydipsia. This is a finding that indicates that the client is experiencing DKA due to the high level of glucose in the blood. Hyperglycemia in DKA can cause polydipsia, which is excessive thirst, due to osmotic diuresis and dehydration.
Full Explanation
Choice A: Rapid pulse. This is not a finding that indicates that the client is experiencing DKA, but rather a sign of hypoglycemia, which is a low level of glucose in the blood. Hypoglycemia can cause rapid pulse due to increased sympathetic nervous system activity and decreased cardiac output.
Choice B: Clammy skin. This is not a finding that indicates that the client is experiencing DKA, but rather a sign of hypoglycemia. Hypoglycemia can cause clammy skin due to increased sweating and vasoconstriction.
Choice C: Choice C: Confusion is commonly found in HHS rather than DKA.
Choice D: Polydipsia. This is a finding that indicates that the client is experiencing DKA due to the high level of glucose in the blood. Hyperglycemia in DKA can cause polydipsia, which is excessive thirst, due to osmotic diuresis and dehydration.