Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A client who is having gastrointestinal (GI) difficulties is undergoing diagnostic procedures.
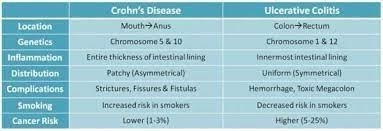
The client asks the nurse about the difference between ulcerative colitis and Crohn's disease.
Which information should the nurse offer?
A. Anal abscess and fistula rarely occur in Crohn's disease.
Incorrect- Anal abscesses and fistulas are more commonly associated with Crohn's disease than with ulcerative colitis. Crohn's disease can involve the entire thickness of the bowel wall and create tunnels or connections (fistulas) between different parts of the gastrointestinal tract.
B. Rectal bleeding is a predominant symptom in ulcerative colitis.
Correct- Rectal bleeding is a common symptom of ulcerative colitis, as the inflamed tissue can bleed easily.
C. Constipation is more common in Crohn's disease.
Incorrect- Constipation is not a common characteristic of Crohn's disease. In fact, both ulcerative colitis and Crohn's disease can lead to a range of bowel habits, including diarrhea and constipation, depending on the extent and location of inflammation.
D. Colitis and Crohn's disease don't involve chronic inflammation of the gastrointestinal tract
Incorrect- Both ulcerative colitis and Crohn's disease are inflammatory bowel diseases (IBD) that involve chronic inflammation of the gastrointestinal tract. Ulcerative colitis primarily affects the colon and rectum, causing continuous areas of inflammation and ulceration. Crohn's disease can affect any part of the gastrointestinal tract, from the mouth to the anus. It often involves patches of inflammation with healthy tissue in between, and it can affect different layers of the bowel wall.
This question is an excerpt from Nurse Dive's nursing test bank - RN Hesi Exit Proctored Exam. Take the full exam now
Full Explanation
A) Incorrect- Anal abscesses and fistulas are more commonly associated with Crohn's disease than with ulcerative colitis. Crohn's disease can involve the entire thickness of the bowel wall and create tunnels or connections (fistulas) between different parts of the gastrointestinal tract.
B) Correct- Rectal bleeding is a common symptom of ulcerative colitis, as the inflamed tissue can bleed easily.
C) Incorrect- Constipation is not a common characteristic of Crohn's disease. In fact, both ulcerative colitis and Crohn's disease can lead to a range of bowel habits, including diarrhea and constipation, depending on the extent and location of inflammation.
D) Incorrect- Both ulcerative colitis and Crohn's disease are inflammatory bowel diseases (IBD) that involve chronic inflammation of the gastrointestinal tract. Ulcerative colitis primarily affects the colon and rectum, causing continuous areas of inflammation and ulceration. Crohn's disease can affect any part of the gastrointestinal tract, from the mouth to the anus. It often involves patches of inflammation with healthy tissue in between, and it can affect different layers of the bowel wall.
Similar Questions
Following morning care, a client with a C-5 spinal cord injury who is sitting in a wheelchair becomes flushed and complains of a headache. Which intervention should the nurse implementfirst?
A. Administer a prescribed PRN dose of hydralazine.
This can be done if initial non-pharmacological interventions do not relieve symptoms, but it is not the first step.
B. Assess the client's blood pressures every 15 minutes.
Monitoring blood pressure is important, but it is secondary to removing the stimulus causing the dysreflexia.
C. Teach the client to recognize the symptoms of dysreflexia.
Incorrect- While education is important for long-term management, the client is currently experiencing symptoms that need immediate attention. The priority is to assess and address the current symptoms.
D. Relieve any kinks or obstruction in the client's Foley tubing.
The client is likely experiencing autonomic dysreflexia, characterized by a sudden and severe increase in blood pressure, flushing, headache, and other symptoms triggered by a noxious stimulus below the level of injury. The first step in managing autonomic dysreflexia is to identify and eliminate the triggering stimulus. For clients with a Foley catheter, a common cause of autonomic dysreflexia is bladder distention due to a kinked or obstructed catheter. Relieving any kinks or obstructions in the Foley tubing can immediately alleviate the symptoms.
Full Explanation
A) This can be done if initial non-pharmacological interventions do not relieve symptoms, but it is not the first step.
B) Monitoring blood pressure is important, but it is secondary to removing the stimulus causing the dysreflexia.
C) Incorrect- While education is important for long-term management, the client is currently experiencing symptoms that need immediate attention. The priority is to assess and address the current symptoms.
D) The client is likely experiencing autonomic dysreflexia, characterized by a sudden and severe increase in blood pressure, flushing, headache, and other symptoms triggered by a noxious stimulus below the level of injury. The first step in managing autonomic dysreflexia is to identify and eliminate the triggering stimulus. For clients with a Foley catheter, a common cause of autonomic dysreflexia is bladder distention due to a kinked or obstructed catheter. Relieving any kinks or obstructions in the Foley tubing can immediately alleviate the symptoms.
The parents are at the bedside and state that each parent thought the other parent was watching the child. They are not sure how long he was in the pool or how he might have fallen in. The temperature of the pool was cool as the temperature outside was about 64 °F (17.8 °C).
Placed a cervical collar with the assistance of the physician. The child's pulse is 121 beats/minute, the airway is patent, and there are no signs of any bleeding.
Review H and P, nurse's note, laboratory results, orders, and imaging studies. What complications should the nurse monitor for in the next 6 to 8 hours? Select all that apply.
A. Cerebral edema
Cerebral edema: Brain injury or trauma can lead to swelling and increased intracranial pressure.
B. Acute asphyxia
Asphyxia is the initial event that occurred in the pool. By the time the child is admitted to the pediatric floor, the asphyxiation event has passed; the nurse now monitors for its aftereffects.
C. Hypertension
Incorrect- Hypertension is not a common complication following near-drowning. The focus should be on potential brain injuries and respiratory distress.
D. Respiratory distress
Correct- Near-drowning can lead to aspiration of water or other substances, which can result in respiratory distress.
E. Hyperthermia
Incorrect- hyperthermia is not likely to occur in this case because the child was exposed to cold water.
F. Subdural hemorrhage
The head CT scan was negative for bleeding. Without a significant traumatic impact or pre-existing condition, a subdural hemorrhage is not a standard complication resulting from a submersion injury.
Full Explanation
Choice A rationale: Hypoxic-ischemic injury from submersion can lead to delayed cerebral edema. Monitoring is critical as the brain's inflammatory response to the initial insult often peaks several hours after the event.
Choice B rationale: Asphyxia is the initial event that occurred in the pool. By the time the child is admitted to the pediatric floor, the asphyxiation event has passed; the nurse now monitors for its aftereffects.
Choice C rationale: Near-drowning victims are more likely to experience hypotension due to myocardial depression or shifting fluid balances. Hypertension is not a typical expected complication in the immediate post-submersion recovery period.
Choice D rationale: Aspiration of water interferes with surfactant production and damages alveolar membranes, leading to pulmonary edema or ARDS. Respiratory status can deteriorate rapidly 6 to 8 hours after the initial insult.
Choice E rationale: The child was in cool water with an outdoor temperature of 64°F, making hypothermia the primary concern. Hyperthermia is not expected unless a secondary infection or a thermregulation failure occurs much later.
Choice F rationale: The head CT scan was negative for bleeding. Without a significant traumatic impact or pre-existing condition, a subdural hemorrhage is not a standard complication resulting from a submersion injury.
The nurse is preparing a client who had a below-the-knee (BKA) amputation for discharge to home. Which recommendation(s) should the nurse provide this client? (Select all that apply.)
A. Inspect skin for redness.
Inspecting the skin for redness is crucial to identify any signs of infection or pressure sores early. Redness can indicate irritation or the beginning of a pressure ulcer, which needs to be addressed promptly to prevent further complications.
B. Use a residual limb shrinker.
Using a residual limb shrinker helps to reduce swelling and shape the residual limb for prosthetic fitting. It also helps in managing pain and promoting healing by providing consistent compression.
C. Avoid range of motion exercises.
Avoiding range of motion exercises is incorrect. Range of motion exercises are essential to maintain joint flexibility and prevent contractures, which can hinder the use of a prosthetic limb.
D. Apply alcohol to the residual limb after bathing.
Applying alcohol to the residual limb after bathing is not recommended. Alcohol can dry out the skin and cause irritation, which can lead to skin breakdown and infection. Instead, the residual limb should be kept clean and moisturized with appropriate skin care products.
Full Explanation
The correct answer is a. Inspect skin for redness and b. Use a residual limb shrinker.
Choice A rationale:
Inspecting the skin for redness is crucial to identify any signs of infection or pressure sores early. Redness can indicate irritation or the beginning of a pressure ulcer, which needs to be addressed promptly to prevent further complications.
Choice B rationale:
Using a residual limb shrinker helps to reduce swelling and shape the residual limb for prosthetic fitting. It also helps in managing pain and promoting healing by providing consistent compression.
Choice C rationale:
Avoiding range of motion exercises is incorrect. Range of motion exercises are essential to maintain joint flexibility and prevent contractures, which can hinder the use of a prosthetic limb.
Choice D rationale:
Applying alcohol to the residual limb after bathing is not recommended. Alcohol can dry out the skin and cause irritation, which can lead to skin breakdown and infection. Instead, the residual limb should be kept clean and moisturized with appropriate skin care products.