Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
(Select all that apply.)
A. Provide diet low in phosphorus.
Providing diet low in phosphorus is not a relevant intervention for a client with cirrhosis of the liver. Phosphorus is a mineral that helps maintain bone health and acid-base balance. Cirrhosis of the liver does not affect phosphorus levels, but it can cause low calcium levels due to impaired vitamin D metabolism. The nurse should provide a diet high in calcium and vitamin D to prevent osteoporosis and fractures.
B. Note signs of swelling and edema.
C. Increase oral fluid intake to 1,500 mL daily.
Increasing oral fluid intake to 1,500 mL daily is not a suitable intervention for a client with cirrhosis of the liver. Fluid intake should be individualized based on the client's fluid status, electrolyte levels, and urine output. Increasing fluid intake may worsen fluid retention and electrolyte imbalance in clients with cirrhosis of the liver. The nurse should restrict fluid intake to 1,000 to 1,500 mL daily or as prescribed by the healthcare provider.
D. Monitor abdominal girth.
E. Report serum albumin and globulin levels.
This question is an excerpt from Nurse Dive's nursing test bank - HESI Exit II Proctored Exam. Take the full exam now
Full Explanation
Choice A reason: Providing diet low in phosphorus is not a relevant intervention for a client with cirrhosis of the liver. Phosphorus is a mineral that helps maintain bone health and acid-base balance. Cirrhosis of the liver does not affect phosphorus levels, but it can cause low calcium levels due to impaired vitamin D metabolism. The nurse should provide a diet high in calcium and vitamin D to prevent osteoporosis and fractures.
Choice C reason: Increasing oral fluid intake to 1,500 mL daily is not a suitable intervention for a client with cirrhosis of the liver. Fluid intake should be individualized based on the client's fluid status, electrolyte levels, and urine output. Increasing fluid intake may worsen fluid retention and electrolyte imbalance in clients with cirrhosis of the liver. The nurse should restrict fluid intake to 1,000 to 1,500 mL daily or as prescribed by the healthcare provider.
Similar Questions
The psychiatric nurse is caring for clients on an adolescent unit. Which client requires the nurse's immediate attention?
A. A 16-year-old client diagnosed with major depression who refuses to participate in group.
A 16-year-old client diagnosed with major depression who refuses to participate in group does not require the nurse's immediate attention. Depression is a mood disorder that causes persistent feelings of sadness, hopelessness, and loss of interest. Refusing to participate in group may indicate low motivation, social withdrawal, or poor self-esteem, which are common symptoms of depression. The nurse should respect the client's preference and offer alternative activities or individual therapy.
B. A 17-year-old client diagnosed with bipolar disorder who is pacing around the lobby.
This client requires immediate intervention because pacing can be a sign of agitation, restlessness, or escalating mania. Clients with bipolar disorder in a manic phase may exhibit increased energy, impulsivity, irritability, and even aggression. If not addressed promptly, this behavior could escalate to disruptive outbursts, impulsive actions, or even violence toward themselves or others. The nurse should intervene by using calm communication, redirection, and possibly medication if prescribed to help de-escalate the situation and ensure safety.
C. An 18-year-old client with antisocial behavior who is being yelled at by other clients.
This scenario involves peer conflict, which is important to address, but it does not necessarily indicate an immediate risk of harm. Clients with antisocial behavior often engage in conflict due to manipulative or confrontational tendencies, but being yelled at does not mean they are in immediate danger. The nurse should monitor the situation and intervene to prevent escalation, but other safety concerns take priority.
D. A 14-year-old client with anorexia nervosa who is refusing to eat the evening snack.
A 14-year-old client with anorexia nervosa who is refusing to eat the evening snack does not require the nurse's immediate attention. Anorexia nervosa is an eating disorder that causes extreme restriction of food intake and fear of weight gain. Refusing to eat the evening snack may indicate distorted body image, dietary rules, or anxiety, which are common factors of anorexia nervosa. The nurse should encourage the client to eat and provide support and education.
E. None
None
F. None
None
Full Explanation
Choice A reason: A 16-year-old client diagnosed with major depression who refuses to participate in group does not require the nurse's immediate attention. Depression is a mood disorder that causes persistent feelings of sadness, hopelessness, and loss of interest. Refusing to participate in group may indicate low motivation, social withdrawal, or poor self-esteem, which are common symptoms of depression. The nurse should respect the client's preference and offer alternative activities or individual therapy.
Choice B reason: This client requires immediate intervention because pacing can be a sign of agitation, restlessness, or escalating mania. Clients with bipolar disorder in a manic phase may exhibit increased energy, impulsivity, irritability, and even aggression. If not addressed promptly, this behavior could escalate to disruptive outbursts, impulsive actions, or even violence toward themselves or others. The nurse should intervene by using calm communication, redirection, and possibly medication if prescribed to help de-escalate the situation and ensure safety.
Choice C reason: This scenario involves peer conflict, which is important to address, but it does not necessarily indicate an immediate risk of harm. Clients with antisocial behavior often engage in conflict due to manipulative or confrontational tendencies, but being yelled at does not mean they are in immediate danger. The nurse should monitor the situation and intervene to prevent escalation, but other safety concerns take priority.
Choice D reason: A 14-year-old client with anorexia nervosa who is refusing to eat the evening snack does not require the nurse's immediate attention. Anorexia nervosa is an eating disorder that causes extreme restriction of food intake and fear of weight gain. Refusing to eat the evening snack may indicate distorted body image, dietary rules, or anxiety, which are common factors of anorexia nervosa. The nurse should encourage the client to eat and provide support and education.
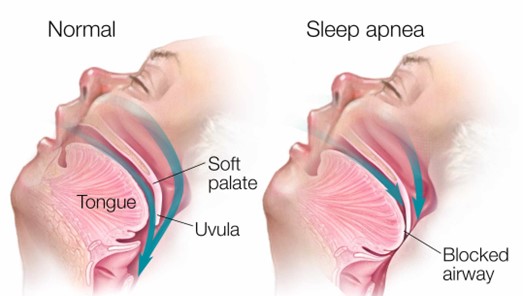
A client with obstructive sleep apnea (OSA) ambulates in the hallway with the nurse prior to bedtime and then returns to bed. Which intervention is most important for the nurse to implement before leaving the client?
A. Apply the client's positive airway pressure device.
This is the correct answer because applying the client's positive airway pressure device is the most important intervention for the nurse to implement before leaving the client. A positive airway pressure device is a treatment that delivers pressurized air through a mask or nasal prongs to keep the upper airway open and prevent apnea episodes during sleep. Obstructive sleep apnea is a condition that causes repeated interruptions in breathing due to partial or complete collapse of the upper airway during sleep. The nurse should ensure that the device is fitted properly and functioning well.
B. Elevate the head of the bed to a 45 degree angle.
Elevating the head of the bed to a 45 degree angle is not a sufficient intervention for the nurse to implement before leaving the client. Elevating the head of the bed can help reduce snoring and improve breathing by preventing the tongue and soft palate from falling back and obstructing the airway. However, it may not be enough to prevent apnea episodes in clients with obstructive sleep apnea, especially if they have other risk factors such as obesity, enlarged tonsils, or nasal congestion. The nurse should also use other interventions such as positive airway pressure device, weight loss, or surgery.
C. Remove dentures or other oral appliances.
Removing dentures or other oral appliances is not a relevant intervention for the nurse to implement before leaving the client. Dentures or other oral appliances are devices that replace missing teeth or improve dental alignment. They may help improve speech, chewing, and appearance, but they do not have a direct impact on obstructive sleep apnea. The nurse should instruct the client to remove dentures or other oral appliances before going to bed to prevent discomfort, infection, or damage.
D. Lift and lock the side rails in place.
Lifting and locking the side rails in place is not a necessary intervention for the nurse to implement before leaving the client. Side rails are bars that attach to the sides of the bed frame to prevent falls or injuries. They may provide safety and security for some clients, but they may also pose risks such as entrapment, strangulation, or agitation. The nurse should assess the need for side rails on an individual basis and consider alternative measures such as bed alarms, low beds, or floor mats.
Full Explanation
Choice B reason: Elevating the head of the bed to a 45-degree angle is not a sufficient intervention for the nurse to implement before leaving the client. Elevating the head of the bed can help reduce snoring and improve breathing by preventing the tongue and soft palate from falling back and obstructing the airway. However, it may not be enough to prevent apnea episodes in clients with obstructive sleep apnea, especially if they have other risk factors such as obesity, enlarged tonsils, or nasal congestion. The nurse should also use other interventions such as a positive airway pressure device, weight loss, or surgery.
Choice C reason: Removing dentures or other oral appliances is not a relevant intervention for the nurse to implement before leaving the client. Dentures or other oral appliances are devices that replace missing teeth or improve dental alignment. They may help improve speech, chewing, and appearance, but they do not have a direct impact on obstructive sleep apnea. The nurse should instruct the client to remove dentures or other oral appliances before going to bed to prevent discomfort, infection, or damage.
Choice D reason: Lifting and locking the side rails in place is not a necessary intervention for the nurse to implement before leaving the client. Side rails are bars that attach to the sides of the bed frame to prevent falls or injuries. They may provide safety and security for some clients, but they may also pose risks such as entrapment, strangulation, or agitation. The nurse should assess the need for side rails on an individual basis and consider alternative measures such as bed alarms, low beds, or floor mats.
A client with influenza needs help in transferring to the bedside commode. The nurse observes the unlicensed assistive personnel (UAP) donning
gloves and a gown to assist the client. Which action should the nurse take?
A. Remind the UAP to apply a fitted respirator mask before entering the client's room.
Reminding the UAP to apply a fitted respirator mask before entering the client's room is not a necessary action for the nurse to take. A respirator mask is a type of personal protective equipment (PPE. that filters out airborne particles and droplets that may contain infectious agents. A respirator mask is required for clients who have or are suspected of having airborne diseases, such as tuberculosis, measles, or chickenpox. Influenza is a respiratory disease that is transmitted by droplet contact, not by airborne contact.
B. Instruct the UAP to notify the nurse of any changes in the client's respiratory status.
Instructing the UAP to notify the nurse of any changes in the client's respiratory status is not a specific action for the nurse to take. Respiratory status is an assessment of the client's breathing pattern, rate, depth, effort, and oxygen saturation. Respiratory status can be affected by various factors, such as infection, inflammation, obstruction, or injury. The nurse should monitor the client's respiratory status regularly and teach the UAP to report any signs or symptoms of respiratory distress, such as dyspnea, cyanosis, wheezes, or cough.
C. Review the need for the UAP to wear a face mask while in close contact with the client.
D. Assign the UAP to provide care for another client and assume full care of the client.
Assigning the UAP to provide care for another client and assuming full care of the client is not a feasible action for the nurse to take. The nurse should delegate tasks according to the scope of practice, competency, and availability of staff. The nurse should not reassign staff without a valid reason or without consulting with other team members. The nurse should also not assume full care of a client unless it is necessary or appropriate. The nurse should supervise and evaluate the UAP's performance and provide feedback and guidance.
Full Explanation
Choice A reason: Reminding the UAP to apply a fitted respirator mask before entering the client's room is not a necessary action for the nurse to take. A respirator mask is a type of personal protective equipment (PPE. that filters out airborne particles and droplets that may contain infectious agents. A respirator mask is required for clients who have or are suspected of having airborne diseases, such as tuberculosis, measles, or chickenpox. Influenza is a respiratory disease that is transmitted by droplet contact, not by airborne contact.
Choice B reason: Instructing the UAP to notify the nurse of any changes in the client's respiratory status is not a specific action for the nurse to take. Respiratory status is an assessment of the client's breathing pattern, rate, depth, effort, and oxygen saturation. Respiratory status can be affected by various factors, such as infection, inflammation, obstruction, or injury. The nurse should monitor the client's respiratory status regularly and teach the UAP to report any signs or symptoms of respiratory distress, such as dyspnea, cyanosis, wheezes, or cough.
Choice D reason: Assigning the UAP to provide care for another client and assuming full care of the client is not a feasible action for the nurse to take. The nurse should delegate tasks according to the scope of practice, competency, and availability of staff. The nurse should not reassign staff without a valid reason or without consulting with other team members. The nurse should also not assume full care of a client unless it is necessary or appropriate. The nurse should supervise and evaluate the UAP's performance and provide feedback and guidance.