Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A client's stool is clay in color. What additional information should the nurse obtain from this client? Select all that apply.
A. History of alcohol abuse
Choice A Reason: History of alcohol abuse is an additional information that the nurse should obtain from this client, as it may indicate liver damage or cirrhosis, which can cause clay-colored stool due to reduced bile production or flow.
B. Intolerance to fatty foods
Choice B Reason: Intolerance to fatty foods is not an additional information that the nurse should obtain from this client, as it does not relate to clay-colored stool, but it may indicate gallbladder disease or malabsorption.
C. Pain in the RUQ radiating to the shoulder.
Choice C Reason: Pain in the RUQ radiating to the shoulder is an additional information that the nurse should obtain from this client, as it may indicate gallstone obstruction or inflammation, which can cause clay-colored stool due to blocked bile ducts.
D. Pain in the McBurney's point
Choice D Reason: Pain in the McBurney's point is not an additional information that the nurse should obtain from this client, as it does not relate to clay-colored stool, but it may indicate appendicitis or diverticulitis.
E. Bleeding ulcer
Choice E Reason: Bleeding ulcer is an additional information that the nurse should obtain from this client, as it may indicate upper gastrointestinal bleeding, which can cause clay-colored stool due to digested blood.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Proctored Exam 3. Take the full exam now
Full Explanation
Choice A Reason: History of alcohol abuse is an additional information that the nurse should obtain from this client, as it may indicate liver damage or cirrhosis, which can cause clay-colored stool due to reduced bile production or flow.
Choice B Reason: Intolerance to fatty foods is not an additional information that the nurse should obtain from this client, as it does not relate to clay-colored stool, but it may indicate gallbladder disease or malabsorption.
Choice C Reason: Pain in the RUQ radiating to the shoulder is an additional information that the nurse should obtain from this client, as it may indicate gallstone obstruction or inflammation, which can cause clay-colored stool due to blocked bile ducts.
Choice D Reason: Pain in the McBurney's point is not an additional information that the nurse should obtain from this client, as it does not relate to clay-colored stool, but it may indicate appendicitis or diverticulitis.
Choice E Reason: Bleeding ulcer is an additional information that the nurse should obtain from this client, as it may indicate upper gastrointestinal bleeding, which can cause clay-colored stool due to digested blood.

Similar Questions
A nurse is caring for a client who had a cholecystectomy and has a T-tube drain. Which of the following actions should the nurse take?
A. Apply a transparent dressing to the drain site.
Reason: Applying a transparent dressing to the drain site is not an appropriate action for the nurse to take, as it may trap moisture and bacteria and increase infection risk.
B. Clamp the tubing when the client ambulates.
Reason: Clamping the tubing when the client ambulates is not an appropriate action for the nurse to take, as it may cause bile accumulation and leakage and increase pressure and pain.
C. Place the client into Fowler's position.
Reason: Placing the client into Fowler's position is an appropriate action for the nurse to take, as it helps to promote drainage and prevent reflux of bile into the liver.
D. Secure the tubing to the client's gown.
Reason: Securing the tubing to the client's gown is not an appropriate action for the nurse to take, as it may cause tension and displacement of the drain and increase discomfort and bleeding.
Full Explanation
Choice A Reason: Applying a transparent dressing to the drain site is not an appropriate action for the nurse to take, as it may trap moisture and bacteria and increase infection risk.
Choice B Reason: Clamping the tubing when the client ambulates is not an appropriate action for the nurse to take, as it may cause bile accumulation and leakage and increase pressure and pain.
Choice C Reason: Placing the client into Fowler's position is an appropriate action for the nurse to take, as it helps to promote drainage and prevent reflux of bile into the liver.
Choice D Reason: Securing the tubing to the client's gown is not an appropriate action for the nurse to take, as it may cause tension and displacement of the drain and increase discomfort and bleeding.
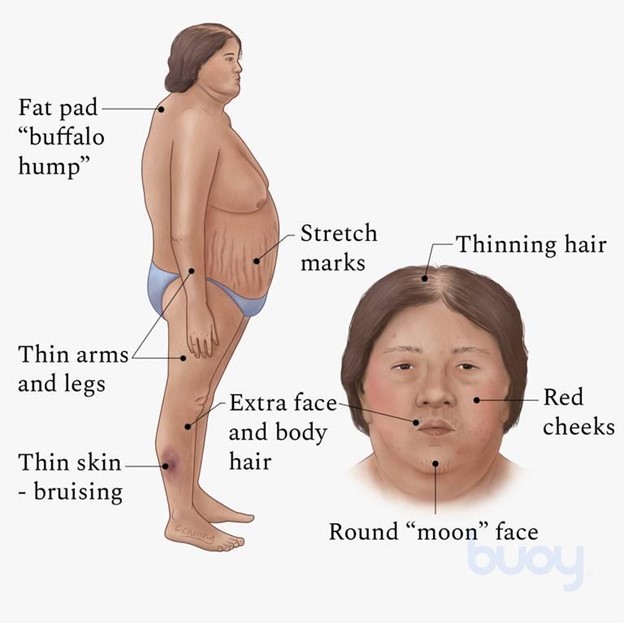
A client admitted to a medical-surgical unit for surgery has a history of Cushing's syndrome. Which physical assessment finding would the nurse expect to observe?
A. Buffalo hump and moon face
Reason: Buffalo hump and moon face are physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, as they indicate fat redistribution and accumulation due to excess cortisol production.
B. Dry, scaly skin and cold intolerance
Reason: Dry, scaly skin and cold intolerance are not physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, but they may indicate hypothyroidism, which affects the metabolism and skin condition.
C. Dry, sticky mucous membranes and hypovolemia
Reason: Dry, sticky mucous membranes and hypovolemia are not physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, but they may indicate dehydration or diabetes insipidus, which affect the fluid balance and urine output.
D. Exophthalmos and tachycardia
Reason: Exophthalmos and tachycardia are not physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, but they may indicate hyperthyroidism, which affects the eye protrusion and heart rate.
Full Explanation
Choice A Reason: Buffalo hump and moon face are physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, as they indicate fat redistribution and accumulation due to excess cortisol production.
Choice B Reason: Dry, scaly skin and cold intolerance are not physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, but they may indicate hypothyroidism, which affects the metabolism and skin condition.
Choice C Reason: Dry, sticky mucous membranes and hypovolemia are not physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, but they may indicate dehydration or diabetes insipidus, which affect the fluid balance and urine output.
Choice D Reason: Exophthalmos and tachycardia are not physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, but they may indicate hyperthyroidism, which affects the eye protrusion and heart rate.
A nurse enters the room of a client with type 1 diabetes mellitus and finds the client difficult to arouse. The client's skin is warm and flushed and the pulse and respiratory rate are increased from the client's baseline. The nurse would first take which action?
A. Assist the RN to prepare an intravenous (IV) insulin infusion.
Reason: Assisting the RN to prepare an IV insulin infusion is not the first action that the nurse should take, as it may not be appropriate for the client's condition without knowing the blood glucose level.
B. Give the client 4 oz of orange juice.
Reason: Giving the client 4 oz of orange juice is not the first action that the nurse should take, as it may worsen the client's condition if the blood glucose level is high.
C. Check the client's capillary blood glucose.
Reason: Checking the client's capillary blood glucose is the first action that the nurse should take, as it helps to determine if the client has hyperglycemia or hypoglycemia and guides the appropriate intervention.
D. Assist the RN to administer 50% dextrose.
Reason: Assisting the RN to administer 50% dextrose is not the first action that the nurse should take, as it may be harmful for the client if the blood glucose level is high.
Full Explanation
Choice A Reason: Assisting the RN to prepare an IV insulin infusion is not the first action that the nurse should take, as it may not be appropriate for the client's condition without knowing the blood glucose level.
Choice B Reason: Giving the client 4 oz of orange juice is not the first action that the nurse should take, as it may worsen the client's condition if the blood glucose level is high.
Choice C Reason: Checking the client's capillary blood glucose is the first action that the nurse should take, as it helps to determine if the client has hyperglycemia or hypoglycemia and guides the appropriate intervention.
Choice D Reason: Assisting the RN to administer 50% dextrose is not the first action that the nurse should take, as it may be harmful for the client if the blood glucose level is high.