Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A college student brings a dorm roommate to the campus clinic because the roommate has been talking to someone who is not present. The client tells the nurse that the voices are saying, "Kill, kill." Which question should the nurse ask the client next?
A. "When did these voices begin?"
B. "Do you believe the voices are real?"
C. "Are you planning to obey the voices?"
It is important to determine if the client has any plans or intentions to act upon the voices' instructions. This information helps gauge the level of risk and guides further interventions and safety measures. While the other questions may also be important to ask during the assessment, determining if the client believes the voices are real and when the voices began can provide valuable information about the client's perception and the duration of the symptoms.
D. "Have you taken any hallucinogens?"
Asking about the use of hallucinogens is relevant to identify potential substance-induced causes of the hallucinations. However, assessing the client's intent and potential for harm is the priority in this situation.
This question is an excerpt from Nurse Dive's nursing test bank - RN Hesi Exit Proctored Exam. Take the full exam now
Full Explanation
It is important to determine if the client has any plans or intentions to act upon the voices' instructions. This information helps gauge the level of risk and guides further interventions and safety measures.
While the other questions may also be important to ask during the assessment, determining if the client believes the voices are real and when the voices began can provide valuable information about the client's perception and the duration of the symptoms. Asking about the use of hallucinogens is relevant to identify potential substance-induced causes of the hallucinations. However, assessing the client's intent and potential for harm is the priority in this situation.
Similar Questions
When planning care for an adolescent with anorexia nervosa, which nursing problem has the highest priority?
A. Disturbed Body Image.
Disturbed Body Image, Interrupted Family Processes, and Noncompliance with treatment regimen are important nursing problems to address, but they are secondary to the client's malnutrition.
B. Interrupted Family Processes.
Disturbed Body Image, Interrupted Family Processes, and Noncompliance with treatment regimen are important nursing problems to address, but they are secondary to the client's malnutrition.
C. Imbalanced Nutrition: less than body requirements.
Less than body requirements would be the nursing problem with the highest priority for an adolescent with anorexia nervosa. Anorexia nervosa is characterized by a severe restriction of food intake leading to a significantly low body weight, which can have serious physical and psychological consequences. Therefore, addressing the client's malnutrition and promoting adequate nutrition intake is crucial to prevent further complications.
D. Noncompliance with treatment regimen.
Disturbed Body Image, Interrupted Family Processes, and Noncompliance with treatment regimen are important nursing problems to address, but they are secondary to the client's malnutrition.
Full Explanation
less than body requirements would be the nursing problem with the highest priority for an adolescent with anorexia nervosa. Anorexia nervosa is characterized by a severe restriction of food intake leading to a significantly low body weight, which can have serious physical and psychological consequences. Therefore, addressing the client's malnutrition and promoting adequate nutrition intake is crucial to prevent further complications.
Disturbed Body Image, Interrupted Family Processes, and Noncompliance with treatment regimen are important nursing problems to address, but they are secondary to the client's malnutrition.
The home care nurse provided self-care instructions for a client with chronic venous insufficiency caused by deep vein thrombosis. Which instruction(s) should the nurse include in the client's discharge teaching plan? (Select all that apply.)
A. Avoid prolonged standing or sitting.
Prolonged standing or sitting can worsen venous insufficiency and increase the risk of blood pooling in the legs. Encouraging the client to move around and avoid prolonged periods of immobility can help improve circulation.
B. Continue wearing compression stockings.
Compression stockings help improve blood flow by applying pressure to the legs, reducing swelling and preventing blood from pooling. The client should be instructed to continue wearing them as prescribed by their healthcare provider.
C. Cross legs at knee but not at ankle.
Crossing the legs can impede blood flow and should be avoided altogether.
D. Use recliner for long periods of sitting.
Sitting for extended periods can also contribute to blood pooling. Using a recliner allows the client to elevate their legs, promoting better circulation and reducing the risk of complications. The nurse should recommend using a recliner when sitting for long periods of time.
E. Maintain the bed flat while sleeping.
Elevating legs during sleep is generally advised to reduce venous pressure.
Full Explanation
A. Prolonged standing or sitting can worsen venous insufficiency and increase the risk of blood pooling in the legs. Encouraging the client to move around and avoid prolonged periods of immobility can help improve circulation.
B. Compression stockings help improve blood flow by applying pressure to the legs, reducing swelling and preventing blood from pooling. The client should be instructed to continue wearing them as prescribed by their healthcare provider.
C.Crossing the legs can impede blood flow and should be avoided altogether.
D. Sitting for extended periods can also contribute to blood pooling. Using a recliner allows the client to elevate their legs, promoting better circulation and reducing the risk of complications. The nurse should recommend using a recliner when sitting for long periods of time.
E. Elevating legs during sleep is generally advised to reduce venous pressure.
An older client with a history of heart failure and admitted to the medical unit after falling at home and has become increasingly confused. The client's spouse is designated as the client's power of attorney.
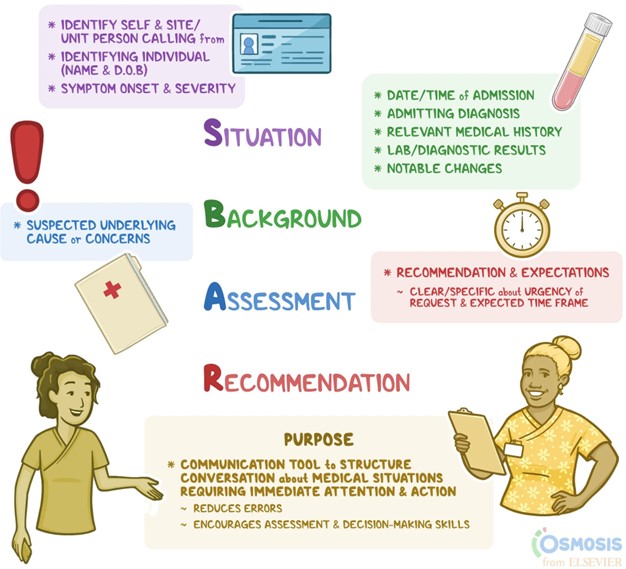
When reporting to the healthcare provider using SBAR (Situation, Background, Assessment, Recommendation) communication, which information should the nurse provide first?
A. Currently prescribed medications.
B. Fall at home as reason for admission.
C. Client's healthcare power of attorney.
D. Increasing confusion of the client.
Situation: Increasing confusion of the client. The nurse should start by providing the current situation, which is the client's increasing confusion. This is crucial information as it indicates a change in the client's condition and may require immediate attention. Background: Fall at home as reason for admission. Next, the nurse should provide the background information, which includes the reason for admission, in this case, the fall at home. This helps the healthcare provider understand the context and potential contributing factors to the client's current condition. Assessment: Currently prescribed medications. After providing the background, the nurse should discuss the assessment findings. In this case, it would be appropriate to mention the client's currently prescribed medications. This information can help the healthcare provider assess for any medication-related issues or interactions that could be contributing to the client's confusion. Recommendation: Client's healthcare power of attorney. Lastly, the nurse should provide the recommendation, which in this case is the client's healthcare power of attorney. This information is important as it identifies the designated decision-maker for the client's healthcare decisions and can assist the healthcare provider in involving the appropriate person in the care planning process.
Full Explanation
Situation: Increasing confusion of the client.
The nurse should start by providing the current situation, which is the client's increasing confusion. This is crucial information as it indicates a change in the client's condition and may require immediate attention.
Background: Fall at home as reason for admission.
Next, the nurse should provide the background information, which includes the reason for admission, in this case, the fall at home. This helps the healthcare provider understand the context and potential contributing factors to the client's current condition. Assessment: Currently prescribed medications.
After providing the background, the nurse should discuss the assessment findings. In this case, it would be appropriate to mention the client's currently prescribed medications. This information can help the healthcare provider assess for any medication-related issues or interactions that could be contributing to the client's confusion.
Recommendation: Client's healthcare power of attorney.
Lastly, the nurse should provide the recommendation, which in this case is the client's healthcare power of attorney. This information is important as it identifies the designated decision-maker for the client's healthcare decisions and can assist the healthcare provider in involving the appropriate person in the care planning process.