Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A few days after a Cerebral Vascular Accident, the patient's family asks the nurse if tissue plasminogen activator (tPA) is a drug therapy option now. The nurse's response based on the knowledge that this drug must be used within:
A. 4 hours
4 hours:This option indicates that tissue plasminogen activator (tPA) must be administered within 4 hours of the onset of stroke symptoms to be considered as a drug therapy option. tPA is a thrombolytic medication used to dissolve blood clots in ischemic stroke, and its effectiveness is highest when administered promptly after the onset of symptoms.
B. 1 hour
1 hour:Administering tPA within 1 hour of stroke onset would be extremely challenging and impractical. It typically takes time for patients to recognize stroke symptoms, seek medical attention, and undergo diagnostic evaluations before tPA administration. While time is of the essence in stroke treatment, 1 hour is too short of a timeframe for most patients to receive tPA.
C. 24 hours
24 hours: Administering tPA beyond 4.5 hours of stroke onset is generally contraindicated due to the increased risk of complications, including hemorrhagic transformation of the stroke. While there may be some extended time windows considered for certain patients under specific circumstances, such as those meeting eligibility criteria for extended thrombolytic therapy, 24 hours is outside the standard timeframe for tPA administration.
D. 8 hours
8 hours:While tPA administration within 8 hours of stroke onset may be feasible for some patients, it is beyond the standard recommended time window for optimal effectiveness. As mentioned earlier, tPA is most effective when administered within the first 3 to 4.5 hours after the onset of symptoms, with earlier administration associated with better outcomes.
This question is an excerpt from Nurse Dive's nursing test bank - Ati Lpn Med Surg Neuro Test 2024 Proctored Exam. Take the full exam now
Full Explanation
A. 4 hours:
This option indicates that tissue plasminogen activator (tPA) must be administered within 4 hours of the onset of stroke symptoms to be considered as a drug therapy option. tPA is a thrombolytic medication used to dissolve blood clots in ischemic stroke, and its effectiveness is highest when administered promptly after the onset of symptoms.
B. 1 hour:
Administering tPA within 1 hour of stroke onset would be extremely challenging and impractical. It typically takes time for patients to recognize stroke symptoms, seek medical attention, and undergo diagnostic evaluations before tPA administration. While time is of the essence in stroke treatment, 1 hour is too short of a timeframe for most patients to receive tPA.
C. 24 hours:
Administering tPA beyond 4.5 hours of stroke onset is generally contraindicated due to the increased risk of complications, including hemorrhagic transformation of the stroke. While there may be some extended time windows considered for certain patients under specific circumstances, such as those meeting eligibility criteria for extended thrombolytic therapy, 24 hours is outside the standard timeframe for tPA administration.
D. 8 hours:
While tPA administration within 8 hours of stroke onset may be feasible for some patients, it is beyond the standard recommended time window for optimal effectiveness. As mentioned earlier, tPA is most effective when administered within the first 3 to 4.5 hours after the onset of symptoms, with earlier administration associated with better outcomes.
Similar Questions
The assessment that indicates a fluid volume excess in a patient in the acute phase of a CVA is:
A. adventitious breath sounds
Adventitious breath sounds:Adventitious breath sounds refer to abnormal lung sounds heard upon auscultation of the chest. These sounds include crackles (rales), wheezes, rhonchi, and pleural friction rubs. In the context of fluid volume excess, particularly in the acute phase of a cerebrovascular accident (CVA) or stroke, adventitious breath sounds such as crackles are indicative of pulmonary edema. Pulmonary edema occurs when there is an excessive accumulation of fluid in the lungs, impairing gas exchange and leading to symptoms such as shortness of breath and respiratory distress.
B. weak pulse
Weak pulse:A weak pulse may suggest poor perfusion or decreased cardiac output rather than fluid volume excess. While decreased cardiac output can be a consequence of heart failure, which may be associated with fluid volume excess, a weak pulse is not a direct indicator of fluid overload. In the acute phase of a CVA, a weak pulse may prompt further assessment for other cardiovascular complications or neurogenic shock.
C. hypotension
Hypotension: Hypotension, or low blood pressure, is not typically associated with fluid volume excess. Instead, hypotension may indicate hypovolemia, shock, or other underlying cardiovascular conditions. While hypotension can occur secondary to severe heart failure or fluid overload in some cases, it is not a direct indicator of fluid volume excess in the acute phase of a CVA.
D. poor skin turgor
Poor skin turgor:Poor skin turgor is a clinical finding associated with dehydration rather than fluid volume excess. In dehydration, the skin loses its elasticity and becomes less resilient when pinched. In contrast, fluid volume excess is characterized by edema, which may manifest as pitting or non-pitting edema, rather than poor skin turgor. However, in fluid volume excess, the skin may appear stretched or taut due to the accumulation of fluid in the interstitial spaces.
Full Explanation
A. Adventitious breath sounds:
Adventitious breath sounds refer to abnormal lung sounds heard upon auscultation of the chest. These sounds include crackles (rales), wheezes, rhonchi, and pleural friction rubs. In the context of fluid volume excess, particularly in the acute phase of a cerebrovascular accident (CVA) or stroke, adventitious breath sounds such as crackles are indicative of pulmonary edema. Pulmonary edema occurs when there is an excessive accumulation of fluid in the lungs, impairing gas exchange and leading to symptoms such as shortness of breath and respiratory distress.
B. Weak pulse:
A weak pulse may suggest poor perfusion or decreased cardiac output rather than fluid volume excess. While decreased cardiac output can be a consequence of heart failure, which may be associated with fluid volume excess, a weak pulse is not a direct indicator of fluid overload. In the acute phase of a CVA, a weak pulse may prompt further assessment for other cardiovascular complications or neurogenic shock.
C. Hypotension:
Hypotension, or low blood pressure, is not typically associated with fluid volume excess. Instead, hypotension may indicate hypovolemia, shock, or other underlying cardiovascular conditions. While hypotension can occur secondary to severe heart failure or fluid overload in some cases, it is not a direct indicator of fluid volume excess in the acute phase of a CVA.
D. Poor skin turgor:
Poor skin turgor is a clinical finding associated with dehydration rather than fluid volume excess. In dehydration, the skin loses its elasticity and becomes less resilient when pinched. In contrast, fluid volume excess is characterized by edema, which may manifest as pitting or non-pitting edema, rather than poor skin turgor. However, in fluid volume excess, the skin may appear stretched or taut due to the accumulation of fluid in the interstitial spaces.
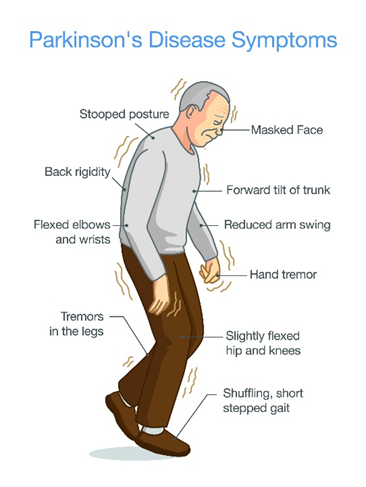
Parkinson's disease has which characteristic symptom(s)? SELECT ALL THAT APPLY
A. Muscle tremors
Muscle tremors:Muscle tremors, particularly resting tremors, are a hallmark feature of Parkinson's disease. These tremors typically occur in the hands, fingers, arms, legs, jaw, or head and may worsen with stress or inactivity.
B. Slow body movement (bradykinesia)
Slow body movement (bradykinesia):Bradykinesia refers to slowness of movement and is another key symptom of Parkinson's disease. Patients may have difficulty initiating movement, experience a decrease in spontaneous movement (hypokinesia), and demonstrate reduced range of motion.
C. Rigidity
Rigidity:Rigidity, or stiffness of the muscles, is a common symptom of Parkinson's disease. It often affects the limbs and trunk and can contribute to difficulty with movement and posture.
D. Pill rolling
Pill rolling:Pill rolling refers to a specific type of tremor characterized by rhythmic, rolling movements of the thumb and fingers, resembling the action of rolling a pill between the fingers and thumb. This tremor is commonly seen in Parkinson's disease.
E. Lack of facial expression
Parkinson's disease can lead to a reduced range of facial expressions, also known as hypomimia or "masked facies." Patients may have a fixed, expressionless facial appearance and reduced blinking.
F. Drooling
Drooling, or excessive salivation, can occur in Parkinson's disease due to impaired swallowing function (dysphagia) and reduced control over oral and facial muscles.
Full Explanation
A. Muscle tremors:
Muscle tremors, particularly resting tremors, are a hallmark feature of Parkinson's disease. These tremors typically occur in the hands, fingers, arms, legs, jaw, or head and may worsen with stress or inactivity.
B. Slow body movement (bradykinesia):
Bradykinesia refers to slowness of movement and is another key symptom of Parkinson's disease. Patients may have difficulty initiating movement, experience a decrease in spontaneous movement (hypokinesia), and demonstrate reduced range of motion.
C. Rigidity:
Rigidity, or stiffness of the muscles, is a common symptom of Parkinson's disease. It often affects the limbs and trunk and can contribute to difficulty with movement and posture.
D. Pill rolling:
Pill rolling refers to a specific type of tremor characterized by rhythmic, rolling movements of the thumb and fingers, resembling the action of rolling a pill between the fingers and thumb. This tremor is commonly seen in Parkinson's disease.
E. Lack of facial expression:
Parkinson's disease can lead to a reduced range of facial expressions, also known as hypomimia or "masked facies." Patients may have a fixed, expressionless facial appearance and reduced blinking.
F. Drooling:
Drooling, or excessive salivation, can occur in Parkinson's disease due to impaired swallowing function (dysphagia) and reduced control over oral and facial muscles.
The nurse is caring for a patient taking a cholinergic agent. When auscultating lung sounds, the nurse notes inspiratory and expiratory wheezing bilaterally. The best action for the nurse to take would be to:
A. withhold the next dose and notify the physician
Withhold the next dose and notify the physician:Withholding the next dose of the cholinergic agent is the appropriate immediate action because the presence of inspiratory and expiratory wheezing bilaterally suggests bronchoconstriction or bronchospasm, which can be a serious adverse reaction to the medication. Notifying the physician promptly allows for further assessment and management of the patient's respiratory symptoms. The physician may need to adjust the medication regimen, order diagnostic tests, or provide treatment for bronchoconstriction.
B. give the next dose
Give the next dose:Administering the next dose of the cholinergic agent could worsen the patient's respiratory symptoms and exacerbate bronchoconstriction. This action is contraindicated in the presence of wheezing, as it may further compromise the patient's respiratory function.
C. assess heart rate
Assess heart rate: While assessing heart rate is an important aspect of patient assessment, it is not the priority in this scenario. The priority is to address the respiratory distress and potential bronchoconstriction associated with the cholinergic agent. Wheezing is a respiratory symptom that suggests airway obstruction, and immediate intervention is necessary to ensure adequate oxygenation and ventilation.
D. assess blood pressure
Assess blood pressure:Similarly, while assessing blood pressure is important in patient care, it is not the priority in this situation. The priority is to address the respiratory distress and potential bronchoconstriction associated with the cholinergic agent. Wheezing indicates respiratory compromise, and prompt action is required to prevent further respiratory deterioration.
Full Explanation
A. Withhold the next dose and notify the physician:
Withholding the next dose of the cholinergic agent is the appropriate immediate action because the presence of inspiratory and expiratory wheezing bilaterally suggests bronchoconstriction or bronchospasm, which can be a serious adverse reaction to the medication. Notifying the physician promptly allows for further assessment and management of the patient's respiratory symptoms. The physician may need to adjust the medication regimen, order diagnostic tests, or provide treatment for bronchoconstriction.
B. Give the next dose:
Administering the next dose of the cholinergic agent could worsen the patient's respiratory symptoms and exacerbate bronchoconstriction. This action is contraindicated in the presence of wheezing, as it may further compromise the patient's respiratory function.
C. Assess heart rate:
While assessing heart rate is an important aspect of patient assessment, it is not the priority in this scenario. The priority is to address the respiratory distress and potential bronchoconstriction associated with the cholinergic agent. Wheezing is a respiratory symptom that suggests airway obstruction, and immediate intervention is necessary to ensure adequate oxygenation and ventilation.
D. Assess blood pressure:
Similarly, while assessing blood pressure is important in patient care, it is not the priority in this situation. The priority is to address the respiratory distress and potential bronchoconstriction associated with the cholinergic agent. Wheezing indicates respiratory compromise, and prompt action is required to prevent further respiratory deterioration.