Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse in a clinic is reviewing the laboratory values of a client who has primary hypothyroidism.
Which of the following laboratory values should the nurse anticipate an elevation of?
A. Free T4
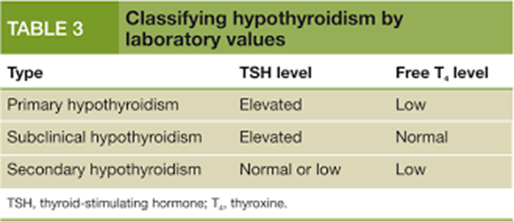
In primary hypothyroidism, the thyroid gland fails to produce sufficient thyroid hormone.Consequently, free T4 levels are typically decreased.
B. Serum T3
Although serum T3 levels may also decrease in primary hypothyroidism due to impaired thyroid function, TSH is the primary marker used for diagnosis and monitoring.
C. Serum T4
Similarly, serum T4 levels may decrease in primary hypothyroidism due to decreased synthesis by the thyroid gland.
D. Thyroid stimulating hormone (TSH)
In primary hypothyroidism, the anterior pituitary gland releases more TSH to stimulate the thyroid gland to produce thyroid hormones. Therefore, elevated TSH levels are characteristic of primary hypothyroidism.
This question is an excerpt from Nurse Dive's nursing test bank - Ati Med Surg Proctored Exam 8. Take the full exam now
Full Explanation
A. In primary hypothyroidism, the thyroid gland fails to produce sufficient thyroid hormone.
Consequently, free T4 levels are typically decreased.
B. Although serum T3 levels may also decrease in primary hypothyroidism due to impaired thyroid function, TSH is the primary marker used for diagnosis and monitoring.
C. Similarly, serum T4 levels may decrease in primary hypothyroidism due to decreased synthesis by the thyroid gland.
D. In primary hypothyroidism, the anterior pituitary gland releases more TSH to stimulate the thyroid gland to produce thyroid hormones. Therefore, elevated TSH levels are characteristic of primary hypothyroidism.
Similar Questions
A nurse is assessing a client who has chronic kidney disease. Which of the following findings is a manifestation of hyperkalemia?
A. Wheezing
Wheezing is not typically associated with hyperkalemia. It can be seen in conditions such as asthma or chronic obstructive pulmonary disease (COPD).
B. Decreased deep tendon reflexes
Hyperkalemia can lead to neuromuscular manifestations, including decreased deep tendon reflexes due to suppression of neuromuscular excitability.
C. Cerebral edema
Cerebral edema is not a typical manifestation of hyperkalemia. It may occur in conditions such as hyponatremia or severe metabolic acidosis.
D. Hypoactive bowel sounds
Gastrointestinal manifestations of hyperkalemia are typically related to smooth muscle involvement and can include hyperactive bowel sounds or diarrhea.
Full Explanation
A. Wheezing is not typically associated with hyperkalemia. It can be seen in conditions such as asthma or chronic obstructive pulmonary disease (COPD).
B. Hyperkalemia can lead to neuromuscular manifestations, including decreased deep tendon reflexes due to suppression of neuromuscular excitability.
C. Cerebral edema is not a typical manifestation of hyperkalemia. It may occur in conditions such as hyponatremia or severe metabolic acidosis.
D. Gastrointestinal manifestations of hyperkalemia are typically related to smooth muscle involvement and can include hyperactive bowel sounds or diarrhea.
A nurse is assessing a client who had a craniotomy and has developed syndrome of inappropriate antidiuretic hormone (SIADH). Which of the following manifestations should the nurse anticipate?
A. Weight loss
SIADH leads to water retention due to excessive secretion of antidiuretic hormone (ADH), resulting in weight gain rather than weight loss.
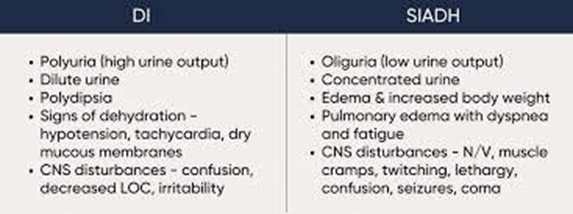
B. Oliguria
SIADH causes the kidneys to retain water, leading to decreased urine output (oliguria) and concentrated urine.
C. Hypernatremia
SIADH typically results in dilutional hyponatremia due to water retention, not hypernatremia.
D. Increased thirst
In SIADH, the body retains water excessively, leading to decreased serum osmolality and suppression of thirst, rather than increased thirst.
Full Explanation
A) SIADH leads to water retention due to excessive secretion of antidiuretic hormone (ADH), resulting in weight gain rather than weight loss.
B) SIADH causes the kidneys to retain water, leading to decreased urine output (oliguria) and concentrated urine.
C) SIADH typically results in dilutional hyponatremia due to water retention, not hypernatremia.
D) In SIADH, the body retains water excessively, leading to decreased serum osmolality and suppression of thirst, rather than increased thirst.
A nurse is caring for a client who has syndrome of inappropriate antidiuretic hormone (SIADH) and a sodium level of 123 mEq/L. Which of the following prescriptions should the nurse anticipate?
A. Maintain an IV of 0.45% sodium chloride.
Infusing hypotonic fluids such as 0.45% sodium chloride can exacerbate hyponatremia in a client with SIADH by further diluting serum sodium levels.
B. Administer desmopressin acetate 0.2 mg orally.
Desmopressin acetate is a synthetic form of ADH and would exacerbate the symptoms of SIADH by increasing water reabsorption and further diluting serum sodium levels.
C. Provide a diet containing 2 g of sodium per day.
Increasing dietary sodium intake would not be appropriate for a client with SIADH, as it would contribute to further fluid retention and exacerbate hyponatremia.
D. Restrict fluid intake to 1,000 mL per day.
Fluid restriction is a key component of managing SIADH to prevent further water retention and dilutional hyponatremia. Restricting fluid intake helps to normalize serum sodium levels by allowing excess water to be excreted.
Full Explanation
A. Infusing hypotonic fluids such as 0.45% sodium chloride can exacerbate hyponatremia in a client with SIADH by further diluting serum sodium levels.
B. Desmopressin acetate is a synthetic form of ADH and would exacerbate the symptoms of SIADH by increasing water reabsorption and further diluting serum sodium levels.
C. Increasing dietary sodium intake would not be appropriate for a client with SIADH, as it would contribute to further fluid retention and exacerbate hyponatremia.
D. Fluid restriction is a key component of managing SIADH to prevent further water retention and dilutional hyponatremia. Restricting fluid intake helps to normalize serum sodium levels by allowing excess water to be excreted.