Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
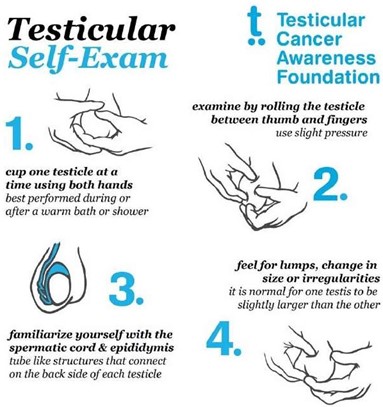
A nurse in a provider’s office is reinforcing teaching with a client about performing testicular self-examination.
Which of the following instructions should the nurse include?
A. “Perform the self-examination every 3 months.”
Choice A is wrong because you should perform the self-examination every month, not every 3 months. This will help you notice any changes over time.
B. “Examine your testicles after a warm shower.”
This is because a warm shower will relax the scrotum and the muscles holding the testicles, making an exam easier. You should gently roll the scrotum with your fingers to feel the surface of each testicle and check for any lumps, bumps, swelling, hardness or other changes.
C. “Palpate both testicles firmly with your fingertips.”
Choice C is wrong because you should not palpate both testicles firmly with your fingertips. You should use a gentle touch and avoid squeezing or pressing too hard.
D. “Apply a cool compress to the scrotum prior to examination.”
Choice D is wrong because you should not apply a cool compress to the scrotum prior to examination. This will make the scrotum contract and tighten, making an exam more difficult.
This question is an excerpt from Nurse Dive's nursing test bank - ATI PN Capstone Proctored Comprehensive Assessment 2020 B. Take the full exam now
Full Explanation
Examine your testicles after a warm shower.
This is because a warm shower will relax the scrotum and the muscles holding the testicles, making an exam easier. You should gently roll the scrotum with your fingers to feel the surface of each testicle and check for any lumps, bumps, swelling, hardness or other changes.
Choice A is wrong because you should perform the self-examination every month, not every 3 months.
This will help you notice any changes over time.
Choice C is wrong because you should not palpate both testicles firmly with your fingertips. You should use a gentle touch and avoid squeezing or pressing too hard.
Choice D is wrong because you should not apply a cool compress to the scrotum prior to examination. This will make the scrotum contract and tighten, making an exam more difficult.
Similar Questions
A nurse is caring for a client who is receiving oxygen via nasal cannula at 4 L/min. Which of the following actions should the nurse take?
A. Avoid the use of humidifiers.
Choice A is wrong because humidifiers can help moisten the dry oxygen and prevent nasal dryness and bleeding. Humidifiers should be used for oxygen flow rates higher than 4 L/min.
B. Position the cannula prongs curving upward in the nose.
Choice B is wrong because the cannula prongs should be positioned curving downward in the nose, not upward. This allows for better alignment with the natural direction of airflow and reduces the risk of dislodgement.
C. Clean the cannula prongs daily.
This is because the nasal cannula can become contaminated with bacteria and mucus, which can cause infection and irritation of the nasal mucosa. Cleaning the cannula prongs daily with soap and water can prevent these complications.
D. Keep the oxygen tubing off the floor.
Choice D is wrong because keeping the oxygen tubing off the floor is not a specific action for nasal cannula use. It is a general safety measure to prevent tripping and contamination of the tubing.
Full Explanation
Clean the cannula prongs daily.

This is because the nasal cannula can become contaminated with bacteria and mucus, which can cause infection and irritation of the nasal mucosa. Cleaning the cannula prongs daily with soap and water can prevent these complications.
Choice A is wrong because humidifiers can help moisten the dry oxygen and prevent nasal dryness and bleeding. Humidifiers should be used for oxygen flow rates higher than 4 L/min.
Choice B is wrong because the cannula prongs should be positioned curving downward in the nose, not upward. This allows for better alignment with the natural direction of airflow and reduces the risk of dislodgement.
Choice D is wrong because keeping the oxygen tubing off the floor is not a specific action for nasal cannula use. It is a general safety measure to prevent tripping and contamination of the tubing.
A nurse on a postpartum unit is caring for a group of clients. Which of the following clients is the nurse’s priority?
A. A client who is 2 days postpartum and whose fundus is 2 to 4 cm below the umbilicus.
Choice A is wrong because a client who is 2 days postpartum and whose fundus is 2 to 4 cm below the umbilicus is showing a normal finding. The fundus should descend about 1 to 2 cm per day after delivery and be nonpalpable by day 10.
B. A client who is 3 days postpartum and has not had a bowel movement since prior to admission.
Choice B is wrong because a client who is 3 days postpartum and has not had a bowel movement since prior to admission is not uncommon. Constipation is a common problem after delivery due to decreased peristalsis, dehydration, and fear of pain. The nurse should encourage fluid intake, fiber intake, and early ambulation to promote bowel function.
C. A client who is 4 days postpartum and has lochia serosa.
Choice C is wrong because a client who is 4 days postpartum and has lochia serosa is also showing a normal finding. Lochia serosa is the pinkish-brown discharge that occurs from day 4 to 10 after delivery. It consists of old blood, serum, leukocytes, and tissue debris.
D. A client who is 1 day postpartum and has not voided in 8 hr.
A client who is 1 day postpartum and has not voided in 8 hr. This client is at risk of urinary retention, bladder distension, and infection due to the effects of epidural anesthesia, perineal trauma, and fluid shifts after delivery. The nurse should assess the client’s bladder and catheterize if necessary.
Full Explanation
A client who is 1 day postpartum and has not voided in 8 hr. This client is at risk of urinary retention, bladder distension, and infection due to the effects of epidural anesthesia, perineal trauma, and fluid shifts after delivery. The nurse should assess the client’s bladder and catheterize if necessary.
Choice A is wrong because a client who is 2 days postpartum and whose fundus is 2 to 4 cm below the umbilicus is showing a normal finding.
The fundus should descend about 1 to 2 cm per day after delivery and be nonpalpable by day 10.
Choice B is wrong because a client who is 3 days postpartum and has not had a bowel movement since prior to admission is not uncommon.
Constipation is a common problem after delivery due to decreased peristalsis, dehydration, and fear of pain.
The nurse should encourage fluid intake, fiber intake, and early ambulation to promote bowel function.
Choice C is wrong because a client who is 4 days postpartum and has lochia serosa is also showing a normal finding.
Lochia serosa is the pinkish-brown discharge that occurs from day 4 to 10 after delivery.
It consists of old blood, serum, leukocytes, and tissue debris.
A nurse is assisting with the care of a client who is in labor with ruptured membranes and has herpes simplex virus with active lesions.
Which of the following actions should the nurse take?
A. Begin an amnioinfusion for the client.
Choice A is wrong because an amnioinfusion is a procedure that involves infusing fluid into the amniotic cavity to increase the volume of amniotic fluid and reduce cord compression. It is not indicated for a client with herpes simplex virus with active lesions.
B. Prepare the client for a cesarean birth.
This is because the client has herpes simplex virus with active lesions, which can be transmitted to the newborn during vaginal delivery and cause serious complications such as neonatal herpes infection. A cesarean birth can prevent this transmission and protect the newborn’s health.
C. Administer ampicillin IV to the client.
Choice C is wrong because ampicillin is an antibiotic that is used to treat bacterial infections, not viral infections such as herpes simplex virus. Ampicillin will not prevent the transmission of herpes simplex virus to the newborn.
D. Initiate an oxytocin infusion for the client.
Choice D is wrong because oxytocin is a hormone that stimulates uterine contractions and can be used to augment or induce labor. It is not indicated for a client with herpes simplex virus with active lesions, as it can increase the risk of transmission to the newborn by prolonging the exposure to infected genital secretions.
Full Explanation
Prepare the client for a cesarean birth.

This is because the client has herpes simplex virus with active lesions, which can be transmitted to the newborn during vaginal delivery and cause serious complications such as neonatal herpes infection. A cesarean birth can prevent this transmission and protect the newborn’s health.
Choice A is wrong because an amnioinfusion is a procedure that involves infusing fluid into the amniotic cavity to increase the volume of amniotic fluid and reduce cord compression.
It is not indicated for a client with herpes simplex virus with active lesions.
Choice C is wrong because ampicillin is an antibiotic that is used to treat bacterial infections, not viral infections such as herpes simplex virus.
Ampicillin will not prevent the transmission of herpes simplex virus to the newborn.
Choice D is wrong because oxytocin is a hormone that stimulates uterine contractions and can be used to augment or induce labor.
It is not indicated for a client with herpes simplex virus with active lesions, as it can increase the risk of transmission to the newborn by prolonging the exposure to infected genital secretions.