Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse in an emergency room is caring for a client who sustained partial-thickness burns to both lower legs, chest, face, and both forearms. Which of the following is the priority action the nurse should take?
A. Administer intravenous pain medication.
Reason: This choice is incorrect because administering intravenous pain medication is not the priority action for a client who has sustained partial-thickness burns. Pain medication may be indicated for pain relief and comfort, but it does not address the potential life-threatening complications of burns such as shock, infection, or respiratory distress.
B. Draw blood for a complete blood cell (CBC) count.
Reason: This choice is incorrect because drawing blood for a CBC count is not the priority action for a client who has sustained partial-thickness burns. A CBC count may be useful to monitor the hematological status and detect any signs of infection or anemia, but it does not address the immediate needs of the client.
C. Insert an indwelling urinary catheter.
Reason: This choice is incorrect because inserting an indwelling urinary catheter is not the priority action for a client who has sustained partial-thickness burns. A urinary catheter may be necessary to measure the urine output and assess the renal function and fluid balance, but it does not address the most urgent problem of the client.
D. Inspect the mouth for signs of inhalation injuries.
Reason: This choice is correct because inspecting the mouth for signs of inhalation injuries is the priority action for a client who has sustained partial-thickness burns. Inhalation injuries are caused by inhaling hot air, smoke, or toxic gases that damage the airway and lungs. They can cause airway obstruction, bronchospasm, pulmonary edema, or respiratory failure. Therefore, the nurse should inspect the mouth for signs such as soot, singed nasal hairs, burns on the lips or tongue, hoarseness, stridor, or wheezes. The nurse should also monitor the oxygen saturation and arterial blood gases to assess the oxygenation and ventilation status of the client.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Custom N235 Final Summer 2023 Proctored Exam. Take the full exam now
Full Explanation
Choice A Reason: This choice is incorrect because administering intravenous pain medication is not the priority action for a client who has sustained partial-thickness burns. Pain medication may be indicated for pain relief and comfort, but it does not address the potential life-threatening complications of burns such as shock, infection, or respiratory distress.
Choice B Reason: This choice is incorrect because drawing blood for a CBC count is not the priority action for a client who has sustained partial-thickness burns. A CBC count may be useful to monitor the hematological status and detect any signs of infection or anemia, but it does not address the immediate needs of the client
Choice C Reason: This choice is incorrect because inserting an indwelling urinary catheter is not the priority action for a client who has sustained partial-thickness burns. A urinary catheter may be necessary to measure the urine output and assess the renal function and fluid balance, but it does not address the most urgent problem of the client.
Choice D Reason: This choice is correct because inspecting the mouth for signs of inhalation injuries is the priority action for a client who has sustained partial-thickness burns. Inhalation injuries are caused by inhaling hot air, smoke, or toxic gases that damage the airway and lungs. They can cause airway obstruction, bronchospasm, pulmonary edema, or respiratory failure. Therefore, the nurse should inspect the mouth for signs such as soot, singed nasal hairs, burns on the lips or tongue, hoarseness, stridor, or wheezes. The nurse should also monitor the oxygen saturation and arterial blood gases to assess the oxygenation and ventilation status of the client.
Similar Questions
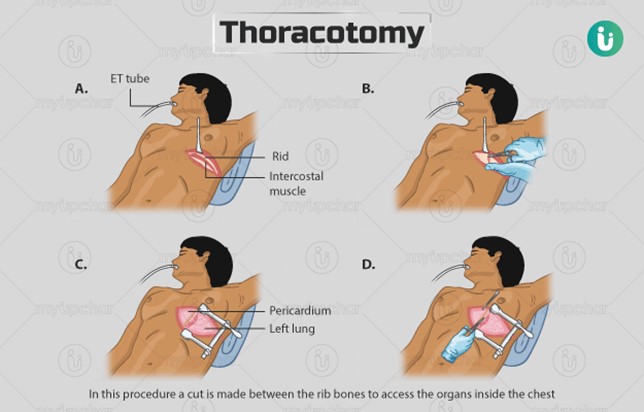
A nurse is observing the closed chest drainage system of a client who is 24 hr post thoracotomy. The nurse notes slow, steady bubbling in the suction control chamber. Which of the following actions should the nurse take?
A. Continue to monitor the client's respiratory status.
Reason: This choice is correct because slow, steady bubbling in the suction control chamber indicates that the suction is working properly and maintaining a negative pressure in the pleural space. The nurse should continue to monitor the client's respiratory status, such as breath sounds, oxygen saturation, and respiratory rate, to assess the effectiveness of the chest drainage system.
B. Check the suction control outlet on the wall.
Reason: This choice is incorrect because checking the suction control outlet on the wall is not necessary unless there is no bubbling in the suction control chamber, which would indicate a problem with the suction source or setting. The nurse should ensure that the suction control outlet is set at the prescribed level, usually between 10 and 20 cm H2O.
C. Clamp the chest tube.
Reason: This choice is incorrect because clamping the chest tube is not indicated unless there is a leak in the system or the chest drainage unit needs to be changed. Clamping the chest tube may cause a buildup of air or fluid in the pleural space, which can lead to tension pneumothorax or pleural effusion.
D. Check the tubing connections for leaks.
Reason: This choice is incorrect because checking the tubing connections for leaks is not necessary unless there is continuous bubbling in the water seal chamber, which would indicate an air leak in the system. The nurse should ensure that all tubing connections are tight and secure, and tape any loose connections.
Full Explanation
Choice A Reason: This choice is correct because slow, steady bubbling in the suction control chamber indicates that the suction is working properly and maintaining a negative pressure in the pleural space. The nurse should continue to monitor the client's respiratory status, such as breath sounds, oxygen saturation, and respiratory rate, to assess the effectiveness of the chest drainage system.
Choice B Reason: This choice is incorrect because checking the suction control outlet on the wall is not necessary unless there is no bubbling in the suction control chamber, which would indicate a problem with the suction source or setting. The nurse should ensure that the suction control outlet is set at the prescribed level, usually between 10 and 20 cm H2O.
Choice C Reason: This choice is incorrect because clamping the chest tube is not indicated unless there is a leak in the system or the chest drainage unit needs to be changed. Clamping the chest tube may cause a buildup of air or fluid in the pleural space, which can lead to tension pneumothorax or pleural effusion.
Choice D Reason: This choice is incorrect because checking the tubing connections for leaks is not necessary unless there is continuous bubbling in the water seal chamber, which would indicate an air leak in the system. The nurse should ensure that all tubing connections are tight and secure, and tape any loose connections.
A nurse is caring for a client who has just developed a pulmonary embolism. Which of the following medications should the nurse anticipate administering?
A. Furosemide
Reason: This choice is incorrect because furosemide is a diuretic that helps to reduce fluid retention and edema. It may be used for clients who have heart failure or hypertension, but it does not treat pulmonary embolism.
B. Heparin
Reason: This choice is correct because heparin is an anticoagulant that helps to prevent blood clots from forming or growing larger. It may be used for clients who have pulmonary embolism, which is a blockage of a pulmonary artery by a blood clot that usually originates from a deep vein thrombosis (DVT). Heparin can reduce the risk of complications such as pulmonary infarction or death.
C. Dexamethasone
Reason: This choice is incorrect because dexamethasone is a corticosteroid that helps to reduce inflammation and immune response. It may be used for clients who have allergic reactions, asthma, or autoimmune diseases, but it does not treat pulmonary embolism.
D. Epinephrine
Reason: This choice is incorrect because epinephrine is a sympathomimetic that helps to stimulate the heart and blood vessels. It may be used for clients who have cardiac arrest, anaphylaxis, or severe asthma, but it does not treat pulmonary embolism.
E. Atropine
Choice E Reason: This choice is incorrect because atropine is an anticholinergic that helps to block the effects of acetylcholine on the heart and smooth muscles. It may be used for clients who have bradycardia, atrioventricular block, or organophosphate poisoning, but it does not treat pulmonary embolism.
Full Explanation
Choice A Reason: This choice is incorrect because furosemide is a diuretic that helps to reduce fluid retention and edema. It may be used for clients who have heart failure or hypertension, but it does not treat pulmonary embolism.
Choice B Reason: This choice is correct because heparin is an anticoagulant that helps to prevent blood clots from forming or growing larger. It may be used for clients who have pulmonary embolism, which is a blockage of a pulmonary artery by a blood clot that usually originates from a deep vein thrombosis (DVT). Heparin can reduce the risk of complications such as pulmonary infarction or death.
Choice C Reason: This choice is incorrect because dexamethasone is a corticosteroid that helps to reduce inflammation and immune response. It may be used for clients who have allergic reactions, asthma, or autoimmune diseases, but it does not treat pulmonary embolism.
Choice D Reason: This choice is incorrect because epinephrine is a sympathomimetic that helps to stimulate the heart and blood vessels. It may be used for clients who have cardiac arrest, anaphylaxis, or severe asthma, but it does not treat pulmonary embolism.
Choice E Reason: This choice is incorrect because atropine is an anticholinergic that helps to block the effects of acetylcholine on the heart and smooth muscles. It may be used for clients who have bradycardia, atrioventricular block, or organophosphate poisoning, but it does not treat pulmonary embolism.
A nurse in the emergency department is caring for a client following an automobile crash in which the client was unrestrained and thrown from the vehicle. When assessing the client, the nurse observes clear fluid draining from the client's nose. Which of the following interventions should the nurse take?
A. Allow the drainage to drip onto a sterile gauze pad.
Reason: This choice is correct because allowing the drainage to drip onto a sterile gauze pad may help to identify if it is cerebrospinal fluid (CSF), which is a clear fluid that surrounds and protects the brain and spinal cord. CSF leakage from the nose (rhinorrhea) may indicate a basilar skull fracture, which is a serious injury that can cause intracranial bleeding, infection, or brain damage. The nurse should test the drainage for the presence of glucose or the halo sign, which are indicators of CSF.
B. Obtain a culture of the specimen using sterile swabs.
Reason: This choice is incorrect because obtaining a culture of the specimen using sterile swabs may introduce bacteria into the nasal cavity and increase the risk of infection. The nurse should avoid inserting anything into the nose or mouth of a client who has a suspected basilar skull fracture.
C. Insert sterile packing into the nares.
Reason: This choice is incorrect because inserting sterile packing into the nares may increase the pressure in the cranial cavity and worsen the injury. The nurse should avoid applying pressure or occluding the nose or ears of a client who has a suspected basilar skull fracture.
D. Suction the nose gently with a bulb syringe.
Reason: This choice is incorrect because suctioning the nose gently with a bulb syringe may damage the nasal mucosa and cause bleeding. The nurse should avoid suctioning or irrigating the nose or ears of a client who has a suspected basilar skull fracture.
Full Explanation
Choice A Reason: This choice is correct because allowing the drainage to drip onto a sterile gauze pad may help to identify if it is cerebrospinal fluid (CSF), which is a clear fluid that surrounds and protects the brain and spinal cord. CSF leakage from the nose (rhinorrhea) may indicate a basilar skull fracture, which is a serious injury that can cause intracranial bleeding, infection, or brain damage. The nurse should test the drainage for the presence of glucose or the halo sign, which are indicators of CSF.
Choice B Reason: This choice is incorrect because obtaining a culture of the specimen using sterile swabs may introduce bacteria into the nasal cavity and increase the risk of infection. The nurse should avoid inserting anything into the nose or mouth of a client who has a suspected basilar skull fracture.
Choice C Reason: This choice is incorrect because inserting sterile packing into the nares may increase the pressure in the cranial cavity and worsen the injury. The nurse should avoid applying pressure or occluding the nose or ears of a client who has a suspected basilar skull fracture.
Choice D Reason: This choice is incorrect because suctioning the nose gently with a bulb syringe may damage the nasal mucosa and cause bleeding. The nurse should avoid suctioning or irrigating the nose or ears of a client who has a suspected basilar skull fracture.
