Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
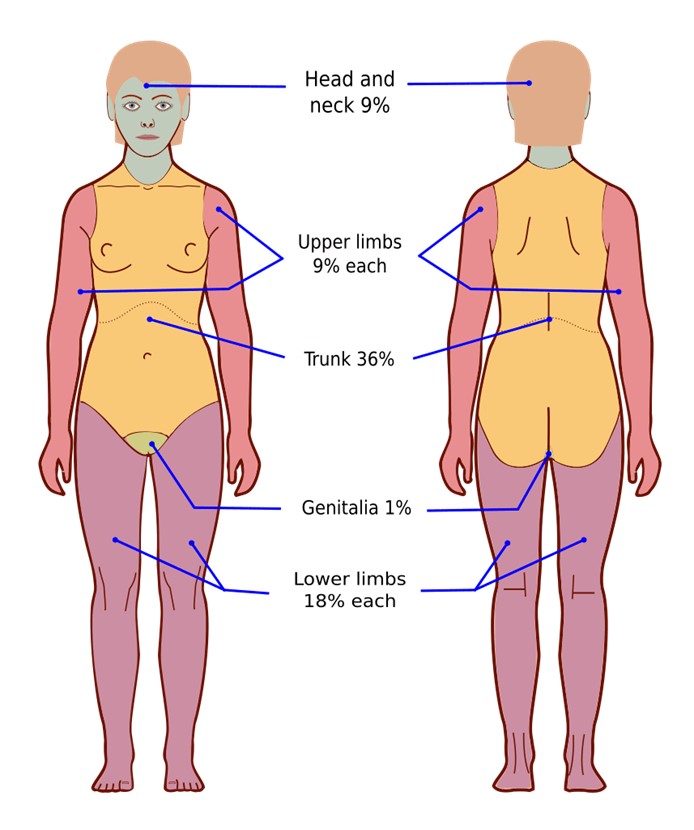
A nurse in the emergency department is caring for a client who has extensive partial and full-thickness burns of the head, neck, and chest. While planning the client's care, the nurse should identify which of the following risks as the priority for assessment and intervention?
A. Infection
Reason: Infection is a serious complication of burn injuries, but not the priority risk for assessment and intervention. The nurse should monitor the client's wound healing, temperature, white blood cell count, and signs of sepsis, and administer antibiotics as prescribed. However, these measures are secondary to ensuring adequate oxygenation and ventilation.
B. Airway obstruction
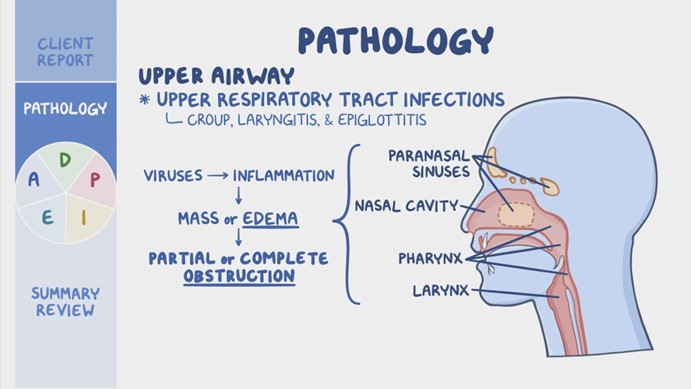
Reason: Airway obstruction is the priority risk for assessment and intervention for a client who has burns of the head, neck, and chest. The nurse should assess the client's airway patency, respiratory rate, oxygen saturation, breath sounds, and signs of respiratory distress, such as stridor, wheezes, or cyanosis. The nurse should also provide humidified oxygen, suction secretions, elevate the head of the bed, and prepare for endotracheal intubation if needed. Airway obstruction can occur due to edema, inflammation, or inhalation injury of the upper airway, and can quickly lead to hypoxia, respiratory failure, and death.
C. Paralytic ileus
Reason: Paralytic ileus is a potential complication of burn injuries, but not the priority risk for assessment and intervention. The nurse should assess the client's bowel sounds, abdominal distension, nausea, vomiting, and stool output, and administer fluids, electrolytes, and nutritional support as prescribed. However, these measures are secondary to ensuring adequate oxygenation and ventilation.
D. Fluid imbalance
Reason: Fluid imbalance is another potential complication of burn injuries, but not the priority risk for assessment and intervention. The nurse should assess the client's fluid status, urine output, vital signs, weight, and serum electrolytes, and administer intravenous fluids as prescribed. However, these measures are secondary to ensuring adequate oxygenation and ventilation.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Custom N235 Final Summer 2023 Proctored Exam. Take the full exam now
Full Explanation
Choice A Reason: Infection is a serious complication of burn injuries, but not the priority risk for assessment and intervention. The nurse should monitor the client's wound healing, temperature, white blood cell count, and signs of sepsis, and administer antibiotics as prescribed. However, these measures are secondary to ensuring adequate oxygenation and ventilation.
Choice B Reason: Airway obstruction is the priority risk for assessment and intervention for a client who has burns of the head, neck, and chest. The nurse should assess the client's airway patency, respiratory rate, oxygen saturation, breath sounds, and signs of respiratory distress, such as stridor, wheezes, or cyanosis. The nurse should also provide humidified oxygen, suction secretions, elevate the head of the bed, and prepare for endotracheal intubation if needed. Airway obstruction can occur due to edema, inflammation, or inhalation injury of the upper airway, and can quickly lead to hypoxia, respiratory failure, and death.
Choice C Reason: Paralytic ileus is a potential complication of burn injuries, but not the priority risk for assessment and intervention. The nurse should assess the client's bowel sounds, abdominal distension, nausea, vomiting, and stool output, and administer fluids, electrolytes, and nutritional support as prescribed. However, these measures are secondary to ensuring adequate oxygenation and ventilation.
Choice D Reason: Fluid imbalance is another potential complication of burn injuries, but not the priority risk for assessment and intervention. The nurse should assess the client's fluid status, urine output, vital signs, weight, and serum electrolytes, and administer intravenous fluids as prescribed. However, these measures are secondary to ensuring adequate oxygenation and ventilation.
Similar Questions
A nurse is caring for a client who had an evacuation of a subdural hematoma. Which of the following actions should the nurse take first?
A. Observe for cerebrospinal fluid (CSF) leaks from the evacuation site.
Reason: Observing for cerebrospinal fluid (CSF) leaks from the evacuation site is important, but not the first action that the nurse should take. CSF leaks can indicate a breach in the dura mater, which can increase the risk of infection and meningitis. The nurse should inspect the dressing and the nose and ears for any clear or bloody drainage, and report any findings to the provider. However, these measures are secondary to ensuring adequate oxygenation and perfusion.
B. Check the oximeter.
Reason: The first action the nurse should take when caring for a client post-evacuation of a subdural hematoma is to check the oximeter to ensure adequate oxygenation. Maintaining proper oxygenation is a priority because hypoxia and hypercapnia can lead to cerebral vasodilation, increasing intracranial pressure (ICP) and worsening neurological outcomes.
C. Assess for an increase in temperature.
Reason: Assessing for an increase in temperature is another important action, but not the first one that the nurse should take. An increase in temperature can indicate an infection, inflammation, or damage to the hypothalamus, which can affect the thermoregulation of the body. The nurse should monitor the temperature and administer antipyretics as prescribed. However, these measures are secondary to ensuring adequate oxygenation and perfusion.
D. Monitor for manifestations of increased intracranial pressure.
Reason: This is crucial, but oxygenation status should be checked first since low oxygen levels can worsen ICP.
Full Explanation
Choice A Reason: Observing for cerebrospinal fluid (CSF) leaks from the evacuation site is important, but not the first action that the nurse should take. CSF leaks can indicate a breach in the dura mater, which can increase the risk of infection and meningitis. The nurse should inspect the dressing and the nose and ears for any clear or bloody drainage, and report any findings to the provider. However, these measures are secondary to ensuring adequate oxygenation and perfusion.
Choice B Reason: The first action the nurse should take when caring for a client post-evacuation of a subdural hematoma is to check the oximeter to ensure adequate oxygenation. Maintaining proper oxygenation is a priority because hypoxia and hypercapnia can lead to cerebral vasodilation, increasing intracranial pressure (ICP) and worsening neurological outcomes. Key Concept: Always prioritize Airway, Breathing, and Circulation (ABCs) when determining the most immediate nursing intervention.
Choice C Reason: Assessing for an increase in temperature is another important action, but not the first one that the nurse should take. An increase in temperature can indicate an infection, inflammation, or damage to the hypothalamus, which can affect the thermoregulation of the body. The nurse should monitor the temperature and administer antipyretics as prescribed. However, these measures are secondary to ensuring adequate oxygenation and perfusion.
Choice D Reason:This is crucial, but oxygenation status should be checked first since low oxygen levels can worsen ICP.
A nurse is caring for a client who had an evacuation of a subdural hematoma. Which of the following actions should the nurse take first?
A. Observe for cerebrospinal fluid (CSF) leaks from the evacuation site.
Reason: Observing for cerebrospinal fluid (CSF) leaks from the evacuation site is important, but not the first action that the nurse should take. CSF leaks can indicate a breach in the dura mater, which can increase the risk of infection and meningitis. The nurse should inspect the dressing and the nose and ears for any clear or bloody drainage, and report any findings to the provider. However, these measures are secondary to ensuring adequate oxygenation and perfusion.
B. Check the oximeter.
Reason: Checking the oximeter is also important, but not the first action that the nurse should take. The oximeter measures the oxygen saturation of the blood, which reflects the adequacy of gas exchange in the lungs. The nurse should maintain the oxygen saturation above 90%, and administer supplemental oxygen as prescribed. However, these measures are secondary to ensuring adequate oxygenation and perfusion.
C. Assess for an increase in temperature.
Reason: Assessing for an increase in temperature is another important action, but not the first one that the nurse should take. An increase in temperature can indicate an infection, inflammation, or damage to the hypothalamus, which can affect the thermoregulation of the body. The nurse should monitor the temperature and administer antipyretics as prescribed. However, these measures are secondary to ensuring adequate oxygenation and perfusion.
D. Monitor for manifestations of increased intracranial pressure.
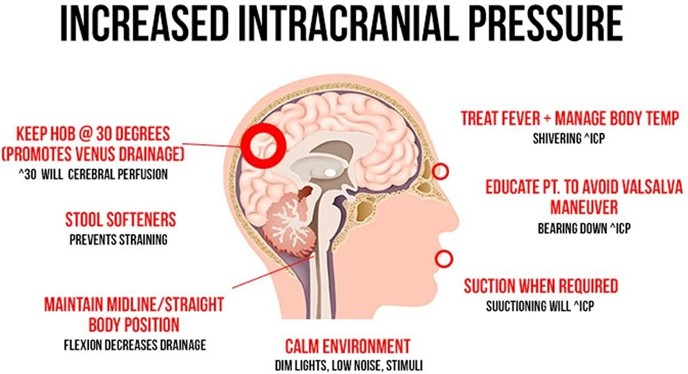
Reason: Monitoring for manifestations of increased intracranial pressure is the first action that the nurse should take. Increased intracranial pressure can result from bleeding, swelling, or fluid accumulation in the brain, which can compress and damage brain tissue and blood vessels. The nurse should assess for signs and symptoms of increased intracranial pressure, such as headache, nausea, vomiting, altered level of consciousness, pupillary changes, or Cushing's triad (bradycardia, hypertension, and irregular respirations). The nurse should also intervene to prevent or reduce increased intracranial pressure, such as elevating the head of the bed, maintaining normothermia, and administering osmotic diuretics. Monitoring for manifestations of increased intracranial pressure is essential to prevent further brain injury and preserve neurological function.
Full Explanation
Choice A Reason: Observing for cerebrospinal fluid (CSF) leaks from the evacuation site is important, but not the first action that the nurse should take. CSF leaks can indicate a breach in the dura mater, which can increase the risk of infection and meningitis. The nurse should inspect the dressing and the nose and ears for any clear or bloody drainage, and report any findings to the provider. However, these measures are secondary to ensuring adequate oxygenation and perfusion.
Choice B Reason: Checking the oximeter is also important, but not the first action that the nurse should take. The oximeter measures the oxygen saturation of the blood, which reflects the adequacy of gas exchange in the lungs. The nurse should maintain the oxygen saturation above 90%, and administer supplemental oxygen as prescribed.
However, these measures are secondary to ensuring adequate oxygenation and perfusion.
Choice C Reason: Assessing for an increase in temperature is another important action, but not the first one that the nurse should take. An increase in temperature can indicate an infection, inflammation, or damage to the hypothalamus, which can affect the thermoregulation of the body. The nurse should monitor the temperature and administer antipyretics as prescribed. However, these measures are secondary to ensuring adequate oxygenation and perfusion.
Choice D Reason: Monitoring for manifestations of increased intracranial pressure is the first action that the nurse should take. Increased intracranial pressure can result from bleeding, swelling, or fluid accumulation in the brain, which can compress and damage brain tissue and blood vessels. The nurse should assess for signs and symptoms of increased intracranial pressure, such as headache, nausea, vomiting, altered level of consciousness, pupillary changes, or Cushing's triad (bradycardia, hypertension, and irregular respirations). The nurse should also intervene to prevent or reduce increased intracranial pressure, such as elevating the head of the bed, maintaining normothermia, and administering osmotic diuretics. Monitoring for manifestations of increased intracranial pressure is essential to prevent further brain injury and preserve neurological function.
A nurse is monitoring a client who was admited with a severe burn injury and is receiving IV fluid resuscitation therapy. The nurse should identify a decrease in which of the following findings as an indication of adequate fluid replacement?
A. Urine output
Reason: Urine output is not a finding that should decrease with adequate fluid replacement. On the contrary, urine output should increase as the fluid therapy restores the renal perfusion and function. The nurse should monitor the urine output and ensure that it is at least 0.5 mL/kg/hr for adults and 1 mL/kg/hr for children.
B. Heart rate
Reason: Heart rate is a finding that should decrease with adequate fluid replacement. A high heart rate is a sign of hypovolemia, which occurs when the burn injury causes fluid loss from the intravascular space. The nurse should monitor the heart rate and expect it to decrease as the fluid therapy replenishes the blood volume and improves the cardiac output.
C. Weight
Reason: Weight is not a finding that should decrease with adequate fluid replacement. On the contrary, weight may increase as the fluid therapy restores the hydration status and corrects the fluid deficit. The nurse should monitor the weight and compare it with the pre-burn weight to evaluate the fluid balance.
D. Blood pressure
Reason: Blood pressure is not a finding that should decrease with adequate fluid replacement. On the contrary, blood pressure may increase as the fluid therapy restores the vascular tone and improves the tissue perfusion. The nurse should monitor the blood pressure and expect it to increase as the fluid therapy compensates for the fluid loss.
Full Explanation
Choice A Reason: Urine output is not a finding that should decrease with adequate fluid replacement. On the contrary, urine output should increase as the fluid therapy restores the renal perfusion and function. The nurse should monitor the urine output and ensure that it is at least 0.5 mL/kg/hr for adults and 1 mL/kg/hr for children.
Choice B Reason: Heart rate is a finding that should decrease with adequate fluid replacement. A high heart rate is a sign of hypovolemia, which occurs when the burn injury causes fluid loss from the intravascular space. The nurse should monitor the heart rate and expect it to decrease as the fluid therapy replenishes the blood volume and improves the cardiac output.
Choice C Reason: Weight is not a finding that should decrease with adequate fluid replacement. On the contrary, weight may increase as the fluid therapy restores the hydration status and corrects the fluid deficit. The nurse should monitor the weight and compare it with the pre-burn weight to evaluate the fluid balance.
Choice D Reason: Blood pressure is not a finding that should decrease with adequate fluid replacement. On the contrary, blood pressure may increase as the fluid therapy restores the vascular tone and improves the tissue perfusion. The nurse should monitor the blood pressure and expect it to increase as the fluid therapy compensates for the fluid loss.