Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is assisting with the plan of care for an older adult client who is 4 hr postoperative following an open reduction and internal fixation of a fractured femur. Which of the following interventions should the nurse include in the plan of care?
A. Maintain the client on bed rest for 72 hr after surgery.
Maintaining the client on bed rest for 72 hr after surgery is not necessarily required for a patient who has undergone an open reduction and internal fixation of a fractured femur. The patient's mobility should be determined by their individual needs and the surgeon's instructions.
B. Check capillary refill in the affected extremity every 4 hr.
Checking capillary refill in the affected extremity every 4 hr is an important intervention for a nurse to include in the plan of care for an older adult client who is 4 hr postoperative following an open reduction and internal fixation of a fractured femur. This helps to monitor the blood flow to the affected extremity and ensure that it is adequate.
C. Restrict oral fluid intake to 1,000 ml per day.
Restricting oral fluid intake to 1,000 ml per day is not necessary for a patient who has undergone an open reduction and internal fixation of a fractured femur. The patient's fluid intake should be determined by their individual needs and any medical conditions they may have.
D. Remove antiembolic stockings once each day to examine skin integrity.
Removing antiembolic stockings once each day to examine skin integrity is not necessarily required for a patient who has undergone an open reduction and internal fixation of a fractured femur. The use of antiembolic stockings and their removal should be determined by the patient's individual needs and the surgeon's instructions.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Custom MS Nurse Proctored Exam. Take the full exam now
Full Explanation
Checking capillary refill in the affected extremity every 4 hr is an important intervention for a nurse to include in the plan of care for an older adult client who is 4 hr postoperative following an open reduction and internal fixation of a fractured femur. This helps to monitor the blood flow to the affected extremity and ensure that it is adequate.
a. Maintaining the client on bed rest for 72 hr after surgery is not necessarily required for a patient who has undergone an open reduction and internal fixation of a fractured femur. The patient's mobility should be determined by their individual needs and the surgeon's instructions.
c. Restricting oral fluid intake to 1,000 ml per day is not necessary for a patient who has undergone an open reduction and internal fixation of a fractured femur. The patient's fluid intake should be determined by their individual needs and any medical conditions they may have.
d. Removing antiembolic stockings once each day to examine skin integrity is not necessarily required for a patient who has undergone an open reduction and internal fixation of a fractured femur. The use of antiembolic stockings and their removal should be determined by the patient's individual needs and the surgeon's instructions.
Similar Questions
A client who has a lower-leg cast reports skin irritation around the upper edge of the cast. Which of the following actions should the nurse take?
A. Suggest that the client use a blunt object such as a comb to relieve the itch.
Suggesting that the client use a blunt object such as a comb to relieve the itch is not recommended as it can cause further irritation or damage to the skin.
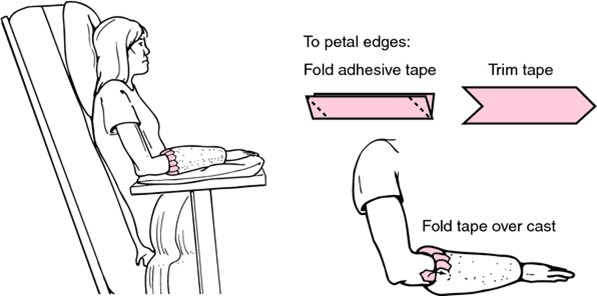
B. Petal the edges of the cast.
If a client reports skin irritation around the upper edge of a lower-leg cast, the nurse should petal the edges of the cast. This involves applying adhesive strips or moleskin around the edges of the cast to smooth them out and prevent them from rubbing against the skin.
C. Tell the client to apply lotion to the irritated skin.
Telling the client to apply lotion to the irritated skin is not recommended as it can cause further irritation or damage to the skin and may also damage the cast.
D. Bivalve the cast.
Bivalving the cast is not necessary for skin irritation around the upper edge of the cast. Bivalving involves cutting the cast in half to relieve pressure and is typically only done in cases of severe swelling or compartment syndrome.
Full Explanation
If a client reports skin irritation around the upper edge of a lower-leg cast, the nurse should petal the edges of the cast. This involves applying adhesive strips or moleskin around the edges of the cast to smooth them out and prevent them from rubbing against the skin.
a. Suggesting that the client use a blunt object such as a comb to relieve the itch is not recommended as it can cause further irritation or damage to the skin.
c. Telling the client to apply lotion to the irritated skin is not recommended as it can cause further irritation or damage to the skin and may also damage the cast.
d. Bivalving the cast is not necessary for skin irritation around the upper edge of the cast. Bivalving involves cutting the cast in half to relieve pressure and is typically only done in cases of severe swelling or compartment syndrome.
A nurse is collecting data from a client who is 6 days post craniotomy for removal of an intracerebral aneurysm. The nurse should monitor the client for which of the following manifestations of increased intracranial pressure?
A. Peripheral edema
Peripheral edema is not a manifestation of increased intracranial pressure. Peripheral edema is swelling in the extremities and can be caused by a variety of conditions.pulses can indicate poor circulation to the feet and can be caused by a variety of conditions.
B. Diarrhea
Diarrhea is not a manifestation of increased intracranial pressure. Diarrhea is loose or watery stools and can be caused by a variety of conditions.
C. Decreased pedal pulses
Decreased pedal pulses are not a manifestation of increased intracranial pressure. Decreased pedal pulses can indicate poor circulation to the feet and can be caused by a variety of conditions.
D. Hypertension
A nurse collecting data from a client who is 6 days post craniotomy for removal of an intracerebral aneurysm should monitor the client for hypertension as a manifestation of increased intracranial pressure. Increased intracranial pressure can cause changes in blood pressure, including hypertension.
Full Explanation
A nurse collecting data from a client who is 6 days post craniotomy for removal of an intracerebral aneurysm should monitor the client for hypertension as a manifestation of increased intracranial pressure. Increased intracranial pressure can cause changes in blood pressure, including hypertension.
a. Peripheral edema is not a manifestation of increased intracranial pressure. Peripheral edema is swelling in the extremities and can be caused by a variety of conditions.
b. Diarrhea is not a manifestation of increased intracranial pressure. Diarrhea is loose or watery stools and
can be caused by a variety of conditions.
c. Decreased pedal pulses are not a manifestation of increased intracranial pressure. Decreased pedal
pulses can indicate poor circulation to the feet and can be caused by a variety of conditions.
A nurse is contributing to the plan of care for a client who is postoperative following a total hip arthroplasty. Which of the following information should the nurse include?
A. Position the lower extremities so that they are touching
Positioning the lower extremities so that they are touching is not necessary for a client who is postoperative following a total hip arthroplasty. The position of the lower extremities should be determined by the surgeon's instructions and the client's comfort.
B. Ensure that the client's heels are touching the bed.
Ensuring that the client's heels are touching the bed is not necessary for a client who is postoperative following a total hip arthroplasty. The position of the heels should be determined by the surgeon's instructions and the client's comfort.
C. Prevent hip flexion of the affected extremity.
When contributing to the plan of care for a client who is postoperative following a total hip arthroplasty, the nurse should include information on preventing hip flexion of the affected extremity. This can help prevent dislocation of the new hip joint and promote healing.
D. Instruct the client to avoid movement of the affected leg.
Instructing the client to avoid movement of the affected leg is not necessary for a client who is postoperative following a total hip arthroplasty. The client will need to begin moving and exercising the affected leg as part of their rehabilitation and recovery.
Full Explanation
When contributing to the plan of care for a client who is postoperative following a total hip arthroplasty, the nurse should include information on preventing hip flexion of the affected extremity. This can help prevent dislocation of the new hip joint and promote healing.
a. Positioning the lower extremities so that they are touching is not necessary for a client who is postoperative following a total hip arthroplasty. The position of the lower extremities should be determined by the surgeon's instructions and the client's comfort.
b. Ensuring that the client's heels are touching the bed is not necessary for a client who is postoperative following a total hip arthroplasty. The position of the heels should be determined by the surgeon's instructions and the client's comfort.
d. Instructing the client to avoid movement of the affected leg is not necessary for a client who is postoperative following a total hip arthroplasty. The client will need to begin moving and exercising the affected leg as part of their rehabilitation and recovery.