Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is caring for a client who has a magnesium level of 3.2 mEq/L. Which of the following medications should the nurse expect to administer?
A. Calcium gluconate
A client with a magnesium level of 3.2 mEq/L has a higher-than-normal magnesium level, indicating hypermagnesemia. The nurse should expect to administer calcium gluconate. Calcium gluconate is the antidote for hypermagnesemia, as it works to antagonize the effects of magnesium on the body. By administering calcium gluconate, the nurse can help counteract the effects of excess magnesium and normalize the client's magnesium levels.
B. Calcitonin
Calcitonin: Calcitonin is not used to treat hypermagnesemia. Calcitonin is a hormone that regulates calcium and phosphorus levels in the body. It is used in certain conditions, such as hypercalcemia (high calcium levels), but it is not indicated for hypermagnesemia.
C. Magnesium oxide
Magnesium oxide: Magnesium oxide is a form of magnesium supplement, and it is not appropriate for a client with hypermagnesemia, as it would further increase the magnesium level, exacerbating the condition.
D. Magnesium sulphate
Magnesium sulphate: Magnesium sulfate is also not appropriate for a client with hypermagnesemia, as it would further elevate the magnesium levels in the body. Magnesium sulfate is often used to treat magnesium deficiency or as a tocolytic agent to prevent premature labor.
This question is an excerpt from Nurse Dive's nursing test bank - RN VATI Pharmacology S 2019 Proctored Exam. Take the full exam now
Full Explanation
A client with a magnesium level of 3.2 mEq/L has a higher-than-normal magnesium level, indicating hypermagnesemia. The nurse should expect to administer calcium gluconate.
Calcium gluconate is the antidote for hypermagnesemia, as it works to antagonize the effects of magnesium on the body. By administering calcium gluconate, the nurse can help counteract the effects of excess magnesium and normalize the client's magnesium levels.
Let's go through the other options:
B. Calcitonin: Calcitonin is not used to treat hypermagnesemia. Calcitonin is a hormone that regulates calcium and phosphorus levels in the body. It is used in certain conditions, such as hypercalcemia (high calcium levels), but it is not indicated for hypermagnesemia.
C. Magnesium oxide: Magnesium oxide is a form of magnesium supplement, and it is not appropriate for a client with hypermagnesemia, as it would further increase the magnesium level, exacerbating the condition.
D. Magnesium sulphate: Magnesium sulfate is also not appropriate for a client with hypermagnesemia, as it would further elevate the magnesium levels in the body. Magnesium sulfate is often used to treat magnesium deficiency or as a tocolytic agent to prevent premature labor.
Similar Questions
A nurse is caring for a client who has congestive heart failure and is taking captopril. Which of the following laboratory values should the nurse report to the provider as a potential adverse effect of captopril?
A. Absolute neutrophil count (ANC) 4.000/ mm^3
Absolute neutrophil count (ANC) 4.000/ mm^3: An absolute neutrophil count of 4.000/ mm^3 is within the normal range, so it is not an adverse effect of captopril that requires immediate reporting.
B. Brain natriuretic peptide (BNP) 90 ng/L
Brain natriuretic peptide (BNP) 90 ng/L: A brain natriuretic peptide (BNP) level of 90 ng/L is used to assess heart failure severity. While BNP levels can be helpful in managing congestive heart failure, a BNP level of 90 ng/L is not an adverse effect of captopril that requires immediate reporting.
C. Sodium 140 mEq/l
Sodium 140 mEq/l: A sodium level of 140 mEq/L is within the normal range, so it is not an adverse effect of captopril that requires immediate reporting.
D. Creatinine 2 mg/dl
The nurse should report a creatinine level of 2 mg/dl to the provider as a potential adverse effect of captopril. Captopril is an angiotensin-converting enzyme (ACE) inhibitor commonly used to treat congestive heart failure and hypertension. One of the side effects of ACE inhibitors, including captopril, is the potential to cause kidney problems, leading to an increase in serum creatinine levels. An increase in serum creatinine may indicate impaired kidney function, and it is essential to monitor kidney function regularly in clients taking ACE inhibitors. Elevated creatinine levels can suggest reduced glomerular filtration rate (GFR) and impaired kidney function, which may require adjustments in medication dosage or further evaluation and management.
Full Explanation
The nurse should report a creatinine level of 2 mg/dl to the provider as a potential adverse effect of captopril. Captopril is an angiotensin-converting enzyme (ACE) inhibitor commonly used to treat congestive heart failure and hypertension. One of the side effects of ACE inhibitors, including captopril, is the potential to cause kidney problems, leading to an increase in serum creatinine levels.
An increase in serum creatinine may indicate impaired kidney function, and it is essential to monitor kidney function regularly in clients taking ACE inhibitors. Elevated creatinine levels can suggest reduced glomerular filtration rate (GFR) and impaired kidney function, which may require adjustments in medication dosage or further evaluation and management.
Let's go through the other options:
A. Absolute neutrophil count (ANC) 4.000/ mm^3: An absolute neutrophil count of 4.000/ mm^3 is within the normal range, so it is not an adverse effect of captopril that requires immediate reporting.
B. Brain natriuretic peptide (BNP) 90 ng/L: A brain natriuretic peptide (BNP) level of 90 ng/L is used to assess heart failure severity. While BNP levels can be helpful in managing congestive heart failure, a BNP level of 90 ng/L is not an adverse effect of captopril that requires immediate reporting.
C. Sodium 140 mEq/l: A sodium level of 140 mEq/L is within the normal range, so it is not an adverse effect of captopril that requires immediate reporting.
A nurse is preparing to administer exenatide for a client who has type 2 diabetes mellitus. Which of the following routes of administration should nurse plan to use?
A. Oral
Oral: Exenatide is not available in an oral form. It is a peptide-based medication that would be destroyed by stomach acid and digestive enzymes if taken orally. Therefore, it must be administered via injection to be effective.
B. intramuscular
Intramuscular: Exenatide is not administered intramuscularly. Intramuscular injections are given deep into the muscle tissue, and exenatide is not formulated or intended for this route of administration.
C. Subcutaneous
Exenatide is a medication used to treat type 2 diabetes mellitus. The nurse should plan to administer exenatide via the subcutaneous route. Subcutaneous administration involves injecting the medication into the fatty tissue just below the skin. Exenatide is available as a subcutaneous injection and is typically given in the abdomen, thigh, or upper arm.
D. intravenous
Intravenous: Exenatide is not administered intravenously. Intravenous injections are given directly into the bloodstream, and exenatide is not suitable for this route of administration.
Full Explanation
Exenatide is a medication used to treat type 2 diabetes mellitus. The nurse should plan to administer exenatide via the subcutaneous route.
Subcutaneous administration involves injecting the medication into the fatty tissue just below the skin. Exenatide is available as a subcutaneous injection and is typically given in the abdomen, thigh, or upper arm.
Let's go through the other options:
A. Oral: Exenatide is not available in an oral form. It is a peptide-based medication that would be destroyed by stomach acid and digestive enzymes if taken orally. Therefore, it must be administered via injection to be effective.
B. Intramuscular: Exenatide is not administered intramuscularly. Intramuscular injections are given deep into the muscle tissue, and exenatide is not formulated or intended for this route of administration.
D. Intravenous: Exenatide is not administered intravenously. Intravenous injections are given directly into the bloodstream, and exenatide is not suitable for this route of administration.
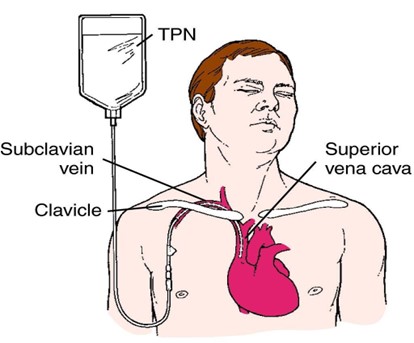
A nurse is planning care for a client who has a new prescription to receive a continuous infusion of total parenteral nutrition (TPN) Which of the following interventions should the nurse implement?
A. Change the TPN infusion tubing once every 3 days
Change the TPN infusion tubing once every 3 days: While changing the TPN infusion tubing regularly is a good practice to maintain asepsis and prevent infection, it is not the priority intervention in this situation. Regularly checking the client's blood glucose level is more crucial to monitor the effects of TPN on blood sugar levels.
B. Check the client's blood glucose level regularly
When caring for a client receiving a continuous infusion of total parenteral nutrition (TPN), the nurse should implement the intervention of checking the client's blood glucose level regularly. TPN is a highly concentrated intravenous nutrition solution containing glucose, amino acids, lipids, vitamins, and minerals, and it is used to provide complete nutrition when the client cannot take oral nutrition. Monitoring blood glucose levels regularly is essential because TPN is rich in glucose, which can significantly affect the client's blood sugar levels. Hyperglycemia (high blood sugar) is a potential complication of TPN infusion. Regular blood glucose monitoring allows the nurse to detect and address any changes in blood sugar levels promptly and to adjust the TPN infusion rate or administer insulin, if necessary, to maintain the client's blood sugar within the target range.
C. Insert the peripheral IV catheter for administration
Insert the peripheral IV catheter for administration: Total parenteral nutrition is a hypertonic solution that can cause irritation and damage to peripheral veins. It is usually administered through a central venous catheter (CVC) placed in a large vein, such as the subclavian or jugular vein. Inserting a peripheral IV catheter for TPN administration is not recommended due to the risk of vein damage and thrombosis.
D. Monitor the client's weight every 3 days
Monitor the client's weight every 3 days: Monitoring the client's weight is an important part of assessing their nutritional status and fluid balance. However, the priority intervention for a client receiving TPN is checking their blood glucose level regularly, as hyperglycemia is a common and significant concern in TPN administration.
Full Explanation
When caring for a client receiving a continuous infusion of total parenteral nutrition (TPN), the nurse should implement the intervention of checking the client's blood glucose level regularly. TPN is a highly concentrated intravenous nutrition solution containing glucose, amino acids, lipids, vitamins, and minerals, and it is used to provide complete nutrition when the client cannot take oral nutrition.
Monitoring blood glucose levels regularly is essential because TPN is rich in glucose, which can significantly affect the client's blood sugar levels. Hyperglycemia (high blood sugar) is a potential complication of TPN infusion. Regular blood glucose monitoring allows the nurse to detect and address any changes in blood sugar levels promptly and to adjust the TPN infusion rate or administer insulin, if necessary, to maintain the client's blood sugar within the target range.
Let's go through the other options:
A. Change the TPN infusion tubing once every 3 days: While changing the TPN infusion tubing regularly is a good practice to maintain asepsis and prevent infection, it is not the priority intervention in this situation. Regularly checking the client's blood glucose level is more crucial to monitor the effects of TPN on blood sugar levels.
C. Insert the peripheral IV catheter for administration: Total parenteral nutrition is a hypertonic solution that can cause irritation and damage to peripheral veins. It is usually administered through a central venous catheter (CVC) placed in a large vein, such as the subclavian or jugular vein. Inserting a peripheral IV catheter for TPN administration is not recommended due to the risk of vein damage and thrombosis.
D. Monitor the client's weight every 3 days: Monitoring the client's weight is an important part of assessing their nutritional status and fluid balance. However, the priority intervention for a client receiving TPN is checking their blood glucose level regularly, as hyperglycemia is a common and significant concern in TPN administration.