Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
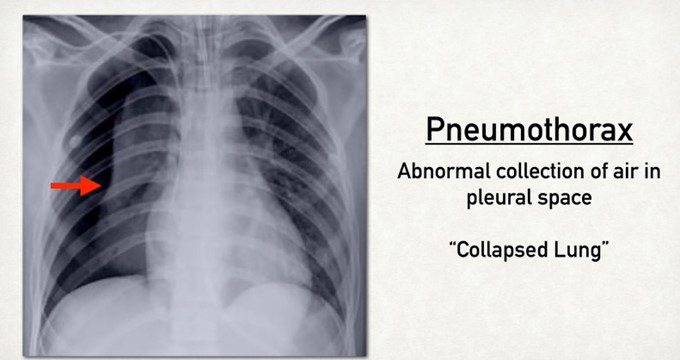
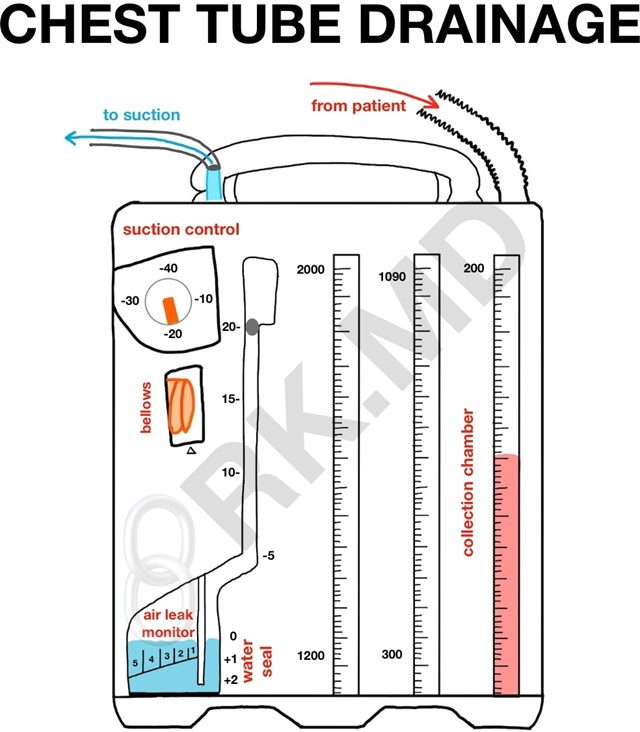
A nurse is caring for a client who has a three-chamber closed chest tube system. Which of the following actions should the nurse take after noticing a rise in the water seal chamber with client inspiration?
A. Immediately notify the provider.
Immediately notifying the provider is not necessary, as a rise in the water seal chamber with client inspiration is not an abnormal or urgent finding. The nurse should only notify the provider if there are signs of complications, such as persistent bubbling in the water seal chamber, which indicates an air leak, or no fluctuation in the water level, which indicates an obstruction or resolution of pneumothorax.
B. Clamp the chest tube near the water seal.
Clamping the chest tube near the water seal is not advisable, as it can cause increased pressure in the pleural space and lead to tension pneumothorax. Clamping the chest tube should only be done for a brief period of time and under specific circumstances, such as changing the drainage system, assessing for an air leak, or preparing for chest tube removal.
C. Continue to monitor the client.
Continuing to monitor the client is the appropriate action for the nurse to take, as a rise in the water seal chamber with client inspiration is a normal and expected finding. The water seal chamber acts as a one-way valve that allows air to exit from the pleural space and prevents air from entering. The water level in this chamber fluctuates with breathing, rising with inspiration and falling with expiration. This indicates that the chest tube system is functioning properly and that there is no air leak.
D. Reposition the client toward the left side.
Repositioning the client toward the left side is not helpful, as it does not affect the water level in the water seal chamber. The nurse should position the client according to their comfort and condition, and avoid placing them flat or on their affected side, as this can impair drainage and ventilation.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Proctored Exam 1. Take the full exam now
Full Explanation
Continuing to monitor the client is the appropriate action for the nurse to take, as a rise in the water seal chamber with client inspiration is a normal and expected finding. The water seal chamber acts as a one-way valve that allows air to exit from the pleural space and prevents air from entering. The water level in this chamber fluctuates with breathing, rising with inspiration and falling with expiration. This indicates that the chest tube system is functioning properly and that there is no air leak.
a) Immediately notifying the provider is not necessary, as a rise in the water seal chamber with client inspiration is not an abnormal or urgent finding. The nurse should only notify the provider if there are signs of complications, such as persistent bubbling in the water seal chamber, which indicates an air leak, or no fluctuation in the water level, which indicates an obstruction or resolution of pneumothorax.
b) Clamping the chest tube near the water seal is not advisable, as it can cause increased pressure in the pleural space and lead to tension pneumothorax. Clamping the chest tube should only be done for a brief period of time and under specific circumstances, such as changing the drainage system, assessing for an air leak, or preparing for chest tube removal.
d) Repositioning the client toward the left side is not helpful, as it does not affect the water level in the water seal chamber. The nurse should position the client according to their comfort and condition, and avoid placing them flat or on their affected side, as this can impair drainage and ventilation.
Similar Questions
A nurse is caring for a client who has emphysema. Which of the following findings should the nurse expect to assess in this client? (Select all that apply.)
A. Dyspnea
Dyspnea, or difficulty breathing, is a common symptom of emphysema, as the client has reduced lung capacity and increased work of breathing. Dyspnea may be worse with exertion, stress, or infection, and may cause anxiety and fatigue. The nurse should monitor the client's respiratory rate, rhythm, depth, and effort, and provide oxygen therapy as prescribed.
B. Barrel chest
Barrel chest, or increased anteroposterior diameter of the chest, is a physical sign of emphysema, as the client has chronic air trapping and hyperinflation of the lungs. Barrel chest may also cause kyphosis, or curvature of the spine, and reduced chest wall movement. The nurse should measure the client's chest circumference and observe for any deformities or asymmetry.
C. Deep respirations
Deep respirations are not expected to be assessed in a client who has emphysema, as the client has shallow and rapid breathing due to air trapping and reduced lung compliance. Deep respirations may indicate other conditions, such as metabolic acidosis or anxiety. The nurse should assess the client's arterial blood gas levels and provide reassurance and relaxation techniques as needed.
D. Clubbing of the fingers
Clubbing of the fingers, or enlargement and rounding of the nail beds, is a late sign of emphysema, as the client has chronic hypoxia and tissue ischemia. Clubbing may also affect the toes and ears, and may indicate pulmonary or cardiac disease. The nurse should inspect the client's nails for shape, color, angle, and capillary refill.
E. Bradycardia
Bradycardia, or slow heart rate, is not expected to be assessed in a client who has emphysema, as the client has tachycardia or normal heart rate due to hypoxia and increased sympathetic stimulation. Bradycardia may indicate other conditions, such as medication side effects, vagal stimulation, or heart block. The nurse should monitor the client's pulse rate, rhythm, quality, and electrocardiogram as indicated.
Full Explanation
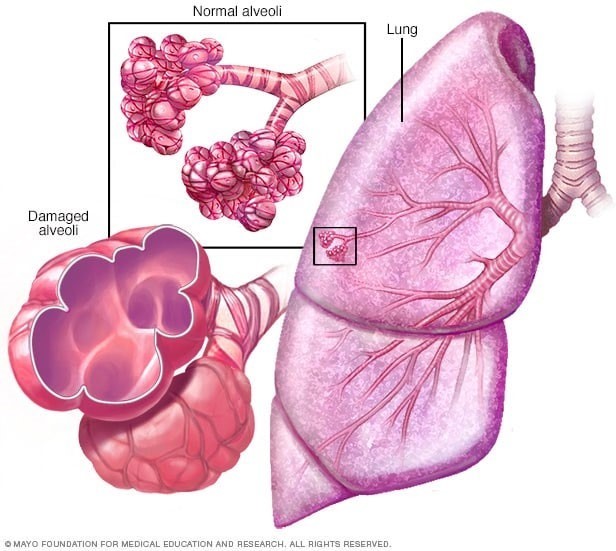
These findings are expected to be assessed in a client who has emphysema, which is a type of chronic obstructive pulmonary disease (COPD) characterized by destruction and enlargement of alveoli, loss of elastic recoil, and air trapping. These changes impair gas exchange and oxygenation, leading to chronic hypoxia and hypercapnia.
a) Dyspnea, or difficulty breathing, is a common symptom of emphysema, as the client has reduced lung capacity and increased work of breathing. Dyspnea may be worse with exertion, stress, or infection, and may cause anxiety and fatigue. The nurse should monitor the client's respiratory rate, rhythm, depth, and effort, and provide oxygen therapy as prescribed.
b) Barrel chest, or increased anteroposterior diameter of the chest, is a physical sign of emphysema, as the client has chronic air trapping and hyperinflation of the lungs. Barrel chest may also cause kyphosis, or curvature of the spine, and reduced chest wall movement. The nurse should measure the client's chest circumference and observe for any deformities or asymmetry.
d) Clubbing of the fingers, or enlargement and rounding of the nail beds, is a late sign of emphysema, as the client has chronic hypoxia and tissue ischemia. Clubbing may also affect the toes and ears, and may indicate pulmonary or cardiac disease. The nurse should inspect the client's nails for shape, color, angle, and capillary refill.
c) Deep respirations are not expected to be assessed in a client who has emphysema, as the client has shallow and rapid breathing due to air trapping and reduced lung compliance. Deep respirations may indicate other conditions, such as metabolic acidosis or anxiety. The nurse should assess the client's arterial blood gas levels and provide reassurance and relaxation techniques as needed.
e) Bradycardia, or slow heart rate, is not expected to be assessed in a client who has emphysema, as the client has tachycardia or normal heart rate due to hypoxia and increased sympathetic stimulation. Bradycardia may indicate other conditions, such as medication side effects, vagal stimulation, or heart block. The nurse should monitor the client's pulse rate, rhythm, quality, and electrocardiogram as indicated.
A nurse is preparing to administer amoxicillin 500 mg PO every 12 hr. The amount available is amoxicillin 250 mg/5 mL suspension. How many mL should the nurse administer?
(Round the answer to the nearest whole number. Use a leading zero if it applies. Do not use a trailing zero.)
Full Explanation
To calculate the amount of mL to administer, the nurse should use the following formula:
(mg ordered / mg available) x mL available = mL to administer
Substituting the values from the question, the nurse should do the following:
(500 mg / 250 mg) x 5 mL = 10 mL
Therefore, the nurse should administer 10 mL of amoxicillin suspension.

A nurse is monitoring a client who has a chest tube in place connected to wall suction due to a right-sided pneumothorax. The client complains of chest burning. Which of the following actions should the nurse take?
A. Increase the client's wall suction.
Increasing the client's wall suction is not advisable, as it can cause increased negative pressure in the pleural space and lead to tension pneumothorax. Increasing the wall suction does not affect the patency of the chest tube or the drainage of air or fluid from the lung. The nurse should maintain the wall suction at the prescribed level and monitor for any changes in the suction chamber.
B. Reposition the client.
Repositioning the client is the appropriate action for the nurse to take, as chest burning may indicate that the chest tube is kinked, twisted, or compressed, which can impair drainage and ventilation. The nurse should gently move the client to a different position and check that the chest tube is not bent or occluded by clothing, bedding, or furniture. The nurse should also ensure that there are no dependent loops or coils in the tubing and that it is secured to prevent dislodgment.
C. Clamp the client's chest tube.
Clamping the client's chest tube is not advisable, as it can cause air or fluid accumulation in the pleural space and lead to tension pneumothorax. Clamping the chest tube does not relieve chest burning or improve drainage or ventilation. The nurse should only clamp the chest tube for a brief period of time and under specific circumstances, such as changing the drainage system, assessing for an air leak, or preparing for chest tube removal.
D. Strip the client's chest tube.
Stripping the client's chest tube is not advisable, as it can cause increased negative pressure in the pleural space and lead to tissue damage or bleeding. Stripping the chest tube involves applying manual pressure along the tubing to force out any clots or debris that may obstruct drainage. However, this practice is not recommended, as it can cause more harm than good. The nurse should only milk the chest tube gently and intermittently if ordered by the provider and if there is evidence of obstruction.
Full Explanation
Repositioning the client is the appropriate action for the nurse to take, as chest burning may indicate that the chest tube is kinked, twisted, or compressed, which can impair drainage and ventilation. The nurse should gently move the client to a different position and check that the chest tube is not bent or occluded by clothing, bedding, or furniture. The nurse should also ensure that there are no dependent loops or coils in the tubing and that it is secured to prevent dislodgment.
a) Increasing the client's wall suction is not advisable, as it can cause increased negative pressure in the pleural space and lead to tension pneumothorax. Increasing the wall suction does not affect the patency of the chest tube or the drainage of air or fluid from the lung. The nurse should maintain the wall suction at the prescribed level and monitor for any changes in the suction chamber.
c) Clamping the client's chest tube is not advisable, as it can cause air or fluid accumulation in the pleural space and lead to tension pneumothorax. Clamping the chest tube does not relieve chest burning or improve drainage or ventilation. The nurse should only clamp the chest tube for a brief period of time and under specific circumstances, such as changing the drainage system, assessing for an air leak, or preparing for chest tube removal.
d) Stripping the client's chest tube is not advisable, as it can cause increased negative pressure in the pleural space and lead to tissue damage or bleeding. Stripping the chest tube involves applying manual pressure along the tubing to force out any clots or debris that may obstruct drainage. However, this practice is not recommended, as it can cause more harm than good. The nurse should only milk the chest tube gently and intermittently if ordered by the provider and if there is evidence of obstruction.