Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is caring for a client who has a vented NG tube set to low intermittent suction and has vomited.
Which of the following actions should the nurse perform first?
A. Replace the NG tube.
Replacing the NG tube might be necessary if it's dislodged or blocked, but it shouldn't be the immediate action. Evaluating the suction device first can help determine if the NG tube itself is the issue or if the problem lies with the suction.
B. Provide oral hygiene care.
Providing oral hygiene care is important for comfort and to prevent aspiration, but it's not the priority intervention in this situation. Addressing the cause of the vomiting, which could be related to suction malfunction, takes precedence.
C. Administer an antiemetic
Administering an antiemetic might be helpful to control nausea and vomiting, but it doesn't address the underlying cause. Evaluating the suction device first is essential to ensure proper gastric decompression and prevent further vomiting episodes.
D. Evaluate functioning of the suction device
Prompt assessment of the suction device is crucial to determine if it's functioning properly.If the suction is inadequate,it can lead to gastric contents accumulating and potentially causing vomiting. Assessing the suction device first allows for timely interventionif it's not working correctly,preventing further complications and discomfort for the client.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Comprehensive Predictor 2023 Exit Proctored Exam A. Take the full exam now
Full Explanation
The correct answer is d. Evaluate functioning of the suction device.
Choice D rationale:
- Prompt assessment of the suction device is crucial to determine if it's functioning properly. If the suction is inadequate, it can lead to gastric contents accumulating and potentially causing vomiting.
- Assessing the suction device first allows for timely intervention if it's not working correctly, preventing further complications and discomfort for the client.
Choice A rationale:
- Replacing the NG tube might be necessary if it's dislodged or blocked, but it shouldn't be the immediate action.
- Evaluating the suction device first can help determine if the NG tube itself is the issue or if the problem lies with the suction.
Choice B rationale:
- Providing oral hygiene care is important for comfort and to prevent aspiration, but it's not the priority intervention in this situation.
- Addressing the cause of the vomiting, which could be related to suction malfunction, takes precedence.
Choice C rationale:
- Administering an antiemetic might be helpful to control nausea and vomiting, but it doesn't address the underlying cause.
- Evaluating the suction device first is essential to ensure proper gastric decompression and prevent further vomiting episodes.
Similar Questions
A nurse is providing teaching to a client who is at 14 weeks of gestation about findings to report to the provider.
Which of the following findings should the nurse include in the teaching
A. Bleeding gums
bleeding gums, is wrong because it is a common occurrence during pregnancy due to hormonal changes that increase blood flow to the gums. It is not a cause for concern unless it is excessive or accompanied by other symptoms.
B. Urinary frequency
urinary frequency, is wrong because it is also a normal finding during pregnancy due to the growing uterus putting pressure on the bladder. It is not a sign of infection or kidney problems unless it is associated with pain, burning, or blood in the urine.
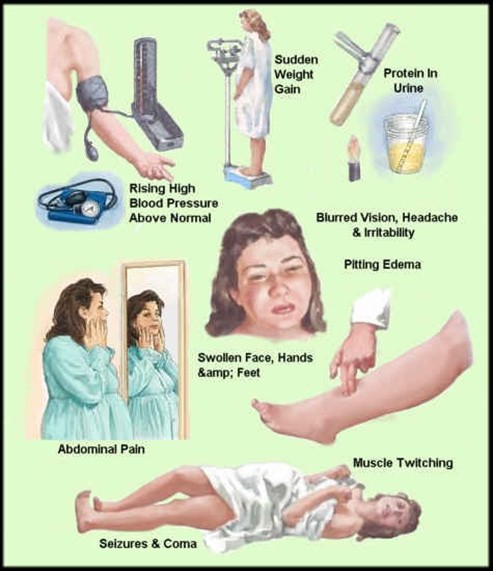
C. preeclampsia
Preeclampsia can affect the placenta, the kidneys, the liver, and the brain of the mother and the fetus. It requires immediate medical attention and may lead to early delivery.
D. faintness upon rising
This is a sign of preeclampsia, a serious complication of pregnancy that can cause high blood pressure, proteinuria, and seizures. faintness upon rising, is wrong because it is usually caused by orthostatic hypotension, a drop in blood pressure when changing positions.
Full Explanation
This is a sign of preeclampsia, a serious complication of pregnancy that can cause high blood pressure, proteinuria, and seizures.
Preeclampsia can affect the placenta, the kidneys, the liver, and the brain of the mother and the fetus. It requires immediate medical attention and may lead to early delivery.
Choice A, bleeding gums, is wrong because it is a common occurrence during pregnancy due to hormonal changes that increase blood flow to the gums. It is not a cause for concern unless it is excessive or accompanied by other symptoms.
Choice B, urinary frequency, is wrong because it is also a normal finding during pregnancy due to the growing uterus putting pressure on the bladder. It is not a sign of infection or kidney problems unless it is associated with pain, burning, or blood in the urine.
Choice D, faintness upon rising, is wrong because it is usually caused by orthostatic hypotension, a drop in blood pressure when changing positions.
This can happen during pregnancy due to the dilation of blood vessels and the increased blood volume. It can be prevented by rising slowly, drinking enough fluids, and avoiding prolonged standing.
A nurse is assessing a client who is experiencing hypovolemia.
Which of the following manifestations should the nurse expect
A. Epistaxis
epistaxis, is wrong because it is not a sign of hypovolemia, but rather a possible cause of it. Epistaxis is a nosebleed that can result from trauma, infection, dryness, or coagulation disorders.
B. Headache
headache, is wrong because it is not a specific sign of hypovolemia, but rather a nonspecific symptom that can have many causes. Headache can be associated with dehydration, but it can also be caused by stress, infection, inflammation, or other factors.
C. Dizziness
Dizziness is a manifestation of hypovolemia, which is a decrease in blood volume due to fluid loss. Hypovolemia can cause orthostatic hypotension, which is a drop in blood pressure when changing positions. This can lead to dizziness, lightheadedness, or fainting.
D. Shortness of breath
shortness of breath, is wrong because it is not a sign of hypovolemia, but rather a sign of fluid volume excess. Fluid volume excess is an increase in blood volume due to fluid retention or overload. Fluid volume excess can cause dyspnea, which is difficulty breathing or shortness of breath. Normal ranges for blood pressure are 90/60 mm Hg to 120/80 mm Hg for adults. Normal ranges for heart rate are 60 to 100 beats per minute for adults.
Full Explanation
, dizziness.
Dizziness is a manifestation of hypovolemia, which is a decrease in blood volume due to fluid loss.
Hypovolemia can cause orthostatic hypotension, which is a drop in blood pressure when changing positions. This can lead to dizziness, lightheadedness, or fainting.
Choice A, epistaxis, is wrong because it is not a sign of hypovolemia, but rather a possible cause of it. Epistaxis is a nosebleed that can result from trauma, infection, dryness, or coagulation disorders.
Choice B, headache, is wrong because it is not a specific sign of hypovolemia, but rather a nonspecific symptom that can have many causes. Headache can be associated with dehydration, but it can also be caused by stress, infection, inflammation, or other factors.
Choice D, shortness of breath, is wrong because it is not a sign of hypovolemia, but rather a sign of fluid volume excess.
Fluid volume excess is an increase in blood volume due to fluid retention or overload. Fluid volume excess can cause dyspnea, which is difficulty breathing or shortness of breath.
Normal ranges for blood pressure are 90/60 mm Hg to 120/80 mm Hg for adults.
Normal ranges for heart rate are 60 to 100 beats per minute for adults.
A nurse is planning care for a client who is scheduled for a thoracentesis.
Which of the following actions should the nurse plan to take
A. Instruct the client to avoid coughing during the procedure
Instruct the client to avoid coughing during the procedure. A thoracentesis is a procedure that involves inserting a needle into the pleural space to remove excess fluid or air. Coughing can increase the risk of pneumothorax (collapsed lung) or bleeding during the procedure.
B. Inform the client that he will be NPO for 6 hr prior to the procedure
is wrong because the client does not need to be NPO (nothing by mouth) for 6 hr prior to the procedure. There is no risk of aspiration during a thoracentesis.
C. Position the client on the affected side for 4 hr following the procedure.
wrong because the client should be positioned on the unaffected side for 4 hr following the procedure. This allows the affected lung to re-expand and prevents fluid from accumulating in the pleural space again.
D. Place the client in the prone position during the procedure
because the client should not be placed in the prone position during the procedure. The prone position makes it difficult to access the pleural space and can compromise breathing.
Full Explanation
The correct answer is choice A. Instruct the client to avoid coughing during the procedure.
A thoracentesis is a procedure that involves inserting a needle into the pleural space to remove excess fluid or air. Coughing can increase the risk of pneumothorax (collapsed lung) or bleeding during the procedure.
Choice B is wrong because the client does not need to be NPO (nothing by mouth) for 6 hr prior to the procedure. There is no risk of aspiration during a thoracentesis.
Choice C is wrong because the client should be positioned on the unaffected side for 4 hr following the procedure. This allows the affected lung to re-expand and prevents fluid from accumulating in the pleural space again.
Choice D is wrong because the client should not be placed in the prone position during the procedure. The prone position makes it difficult to access the pleural space and can compromise breathing.