Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is caring for a client who is at 38 weeks of gestation and is experiencing continuous abdominal pain and vaginal bleeding. The client has a history of cocaine use. The nurse should identify that the client is likely experiencing which of the following complications?
A. Abruptio placentae.
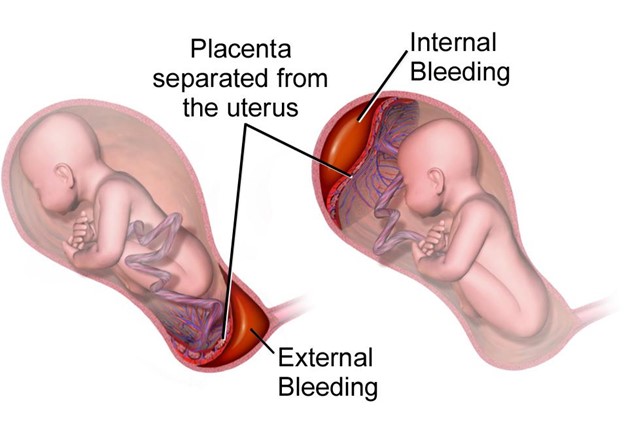
Continuous abdominal pain and vaginal bleeding in a client with a history of cocaine use are indicative of abruptio placentae. Abruptio placentae is a medical emergency where the placenta detaches from the uterine wall before delivery, leading to severe bleeding and abdominal pain. Immediate medical intervention is necessary to prevent complications for both the mother and the baby.
B. Hydatidiform mole.
Hydatidiform mole is a gestational trophoblastic disease that occurs due to an abnormal pregnancy. It is not associated with continuous abdominal pain and vaginal bleeding. Instead, clients with this condition often present with vaginal bleeding and a grape-like cluster of cysts in the uterus.
C. Preterm labor.
Preterm labor involves regular uterine contractions and cervical changes before 37 weeks of gestation. While preterm labor can cause abdominal discomfort, it is not usually described as continuous abdominal pain. Vaginal bleeding is not a typical symptom of preterm labor.
D. Placenta previa.
Placenta previa is a condition where the placenta covers the opening of the cervix. It can cause painless vaginal bleeding, but it is not usually associated with continuous abdominal pain. Clients with placenta previa often experience sudden, painless bleeding later in pregnancy.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Maternal Newborn Proctored Exam. Take the full exam now
Full Explanation
Choice A rationale:
Continuous abdominal pain and vaginal bleeding in a client with a history of cocaine use are indicative of abruptio placentae. Abruptio placentae is a medical emergency where the placenta detaches from the uterine wall before delivery, leading to severe bleeding and abdominal pain. Immediate medical intervention is necessary to prevent complications for both the mother and the baby.
Choice B rationale:
Hydatidiform mole is a gestational trophoblastic disease that occurs due to an abnormal pregnancy. It is not associated with continuous abdominal pain and vaginal bleeding. Instead, clients with this condition often present with vaginal bleeding and a grape-like cluster of cysts in the uterus.
Choice C rationale:
Preterm labor involves regular uterine contractions and cervical changes before 37 weeks of gestation. While preterm labor can cause abdominal discomfort, it is not usually described as continuous abdominal pain. Vaginal bleeding is not a typical symptom of preterm labor.
Choice D rationale:
Placenta previa is a condition where the placenta covers the opening of the cervix. It can cause painless vaginal bleeding, but it is not usually associated with continuous abdominal pain. Clients with placenta previa often experience sudden, painless bleeding later in pregnancy.
Similar Questions
A nurse is caring for a client who is at 38 weeks of gestation and is experiencing continuous abdominal pain and vaginal bleeding. The client has a history of cocaine use. The nurse should identify that the client is likely experiencing which of the following complications?
A. Abruptio placentae.
The client is experiencing continuous abdominal pain and vaginal bleeding, which are key signs of abruptio placentae. This condition occurs when the placenta prematurely separates from the uterine wall before the baby is born, leading to bleeding and potential fetal distress. The history of cocaine use can be a risk factor for abruptio placentae, as cocaine use may lead to vasoconstriction and reduced blood flow to the placenta.
B. Hydatidiform mole.
Hydatidiform mole is not likely in this case because it presents with symptoms such as vaginal bleeding and a "grape-like” mass on ultrasound. The continuous abdominal pain is not typical for a hydatidiform mole.
C. Preterm labor.
Preterm labor is not the likely complication in this scenario because the client is at 38 weeks of gestation, which is considered full term. Preterm labor refers to labor that occurs before 37 weeks of gestation.
D. Placenta previa.
Placenta previa is not the likely complication as it presents with painless vaginal bleeding in the third trimester, and the abdominal pain described in the question suggests a different condition.
Full Explanation
Choice A rationale:
The client is experiencing continuous abdominal pain and vaginal bleeding, which are key signs of abruptio placentae. This condition occurs when the placenta prematurely separates from the uterine wall before the baby is born, leading to bleeding and potential fetal distress. The history of cocaine use can be a risk factor for abruptio placentae, as cocaine use may lead to vasoconstriction and reduced blood flow to the placenta.
Choice B rationale:
Hydatidiform mole is not likely in this case because it presents with symptoms such as vaginal bleeding and a "grape-like” mass on ultrasound. The continuous abdominal pain is not typical for a hydatidiform mole.
Choice C rationale:
Preterm labor is not the likely complication in this scenario because the client is at 38 weeks of gestation, which is considered full term. Preterm labor refers to labor that occurs before 37 weeks of gestation.
Choice D rationale:
Placenta previa is not the likely complication as it presents with painless vaginal bleeding in the third trimester, and the abdominal pain described in the question suggests a different condition.
A nurse is teaching a client who is to start using a diaphragm for contraception. Which of the following client statements indicates an understanding of the teaching?
A. "I will leave the diaphragm in place for 4 hours following intercourse.”
Leaving the diaphragm in place for 4 hours following intercourse is incorrect. The diaphragm should be left in place for at least 6 hours after intercourse to ensure effectiveness in preventing pregnancy.
B. "I will remove the diaphragm by catching the rim below the dome with my forefinger.”
Removing the diaphragm by catching the rim below the dome with the forefinger is incorrect. The diaphragm should be removed by hooking the finger behind the rim to avoid damaging the dome and ensure proper removal.
C. "I will place a thin layer of mineral oil on the diaphragm once per week.”
Placing a thin layer of mineral oil on the diaphragm once per week is incorrect. Mineral oil can weaken latex diaphragms, reducing their effectiveness. Water-based lubricants are recommended for use with diaphragms.
D. "I will place 2 teaspoons of spermicide on the inside of the diaphragm before inserting it.”
Placing 2 teaspoons of spermicide on the inside of the diaphragm before insertion is the correct technique. Spermicide helps to immobilize and kill sperm, enhancing the contraceptive effect of the diaphragm.
Full Explanation
Choice A rationale:
Leaving the diaphragm in place for 4 hours following intercourse is incorrect. The diaphragm should be left in place for at least 6 hours after intercourse to ensure effectiveness in preventing pregnancy.
Choice B rationale:
Removing the diaphragm by catching the rim below the dome with the forefinger is incorrect. The diaphragm should be removed by hooking the finger behind the rim to avoid damaging the dome and ensure proper removal.
Choice C rationale:
Placing a thin layer of mineral oil on the diaphragm once per week is incorrect. Mineral oil can weaken latex diaphragms, reducing their effectiveness. Water-based lubricants are recommended for use with diaphragms.
Choice D rationale:
Placing 2 teaspoons of spermicide on the inside of the diaphragm before insertion is the correct technique. Spermicide helps to immobilize and kill sperm, enhancing the contraceptive effect of the diaphragm.
A nurse is caring for a client who is in active labor and notes late decelerations in the FHR on the external fetal monitor. Which of the following actions should the nurse take first?
A. Change the client's position.
When late decelerations are noted in the fetal heart rate (FHR) tracing, it indicates that the fetal oxygen supply may be compromised. The nurse should first change the client's position, such as moving her to the left lateral position or a hands-and-knees position, to improve uteroplacental blood flow and relieve pressure on the vena cava.
B. Palpate the uterus to assess for tachysystole.
Palpating the uterus to assess for tachysystole is not the priority action when late decelerations are observed. Tachysystole refers to excessively frequent uterine contractions and may contribute to fetal distress, but the immediate concern is addressing the decelerations.
C. Increase the client's IV infusion rate.
Increasing the client's IV infusion rate may not address the underlying cause of late decelerations. While maintaining hydration is important, it's not the first action to take in this situation.
D. Administer oxygen at 10 L/min via a nonrebreather mask.
Administering oxygen at 10 L/min via a non-rebreather mask may be beneficial for the client and fetus, but it is not the first action to take. The nurse should address the position change first to improve oxygenation through better blood flow before considering supplemental oxygen.
Full Explanation
Choice A rationale:
When late decelerations are noted in the fetal heart rate (FHR) tracing, it indicates that the fetal oxygen supply may be compromised. The nurse should first change the client's position, such as moving her to the left lateral position or a hands-and-knees position, to improve uteroplacental blood flow and relieve pressure on the vena cava.
Choice B rationale:
Palpating the uterus to assess for tachysystole is not the priority action when late decelerations are observed. Tachysystole refers to excessively frequent uterine contractions and may contribute to fetal distress, but the immediate concern is addressing the decelerations.
Choice C rationale:
Increasing the client's IV infusion rate may not address the underlying cause of late decelerations. While maintaining hydration is important, it's not the first action to take in this situation.
Choice D rationale:
Administering oxygen at 10 L/min via a non-rebreather mask may be beneficial for the client and fetus, but it is not the first action to take. The nurse should address the position change first to improve oxygenation through better blood flow before considering supplemental oxygen.