Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is caring for a client who is at risk for shock. Which of the following findings is the earliest indicator that this complication is developing?
A. Decreased level of consciousness
Reason: This is incorrect because a decreased level of consciousness is a late sign of shock, not an early one. Decreased level of consciousness indicates that the brain is not receiving enough oxygen and blood flow, which can lead to irreversible damage and death.
B. Increased respiratory rate
Reason: This is correct because increased respiratory rate is an early sign of shock, indicating hypoxia. This finding indicates that the client is experiencing hypoxia, which is a lack of oxygen in the tissues and organs. Hypoxia is a common and early sign of shock, which is a condition where the body's vital organs do not receive enough blood flow and oxygen due to low blood pressure, low cardiac output, or low blood volume. The client's respiratory rate increases as a compensatory mechanism to increase oxygen intake and delivery.
C. Hypotension
Reason: This is incorrect because hypotension is a late sign of shock, not an early one. Hypotension indicates that the blood pressure is too low to maintain adequate perfusion and oxygenation to the vital organs.
D. Anuria
Reason: This is incorrect because anuria is a late sign of shock, not an early one. Anuria indicates that the kidneys are not receiving enough blood flow and oxygen, which can result in acute kidney injury or failure.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg 2 Proctored Exam. Take the full exam now
Full Explanation
Choice A Reason: This is incorrect because a decreased level of consciousness is a late sign of shock, not an early one. Decreased level of consciousness indicates that the brain is not receiving enough oxygen and blood flow, which can lead to irreversible damage and death.
Choice B Reason: This is correct because increased respiratory rate is an early sign of shock, indicating hypoxia. This finding indicates that the client is experiencing hypoxia, which is a lack of oxygen in the tissues and organs. Hypoxia is a common and early sign of shock, which is a condition where the body's vital organs do not receive enough blood
flow and oxygen due to low blood pressure, low cardiac output, or low blood volume. The client's respiratory rate increases as a compensatory mechanism to increase oxygen intake and delivery.
Choice C Reason: This is incorrect because hypotension is a late sign of shock, not an early one. Hypotension indicates that the blood pressure is too low to maintain adequate perfusion and oxygenation to the vital organs.
Choice D Reason: This is incorrect because anuria is a late sign of shock, not an early one. Anuria indicates that the kidneys are not receiving enough blood flow and oxygen, which can result in acute kidney injury or failure.
Similar Questions
A nurse in a cardiac care unit is caring for a client with acute right-sided heart failure. Which of the following findings should the nurse expect?
A. Decreased specific gravity
Decreased specific gravity is not a finding of right-sided heart failure. Specific gravity is a measure of urine concentration, which can be affected by fluid intake, dehydration, kidney function, and diuretic use. Right-sided heart failure does not directly affect urine concentration, but it can cause fluid retention and edema in the body.
B. Decreased brain natriuretic peptide (BNP)
Decreased brain natriuretic peptide (BNP) is not a finding of right-sided heart failure. BNP is a hormone that is released by the heart when it is stretched or overloaded. BNP helps to lower blood pressure and reduce fluid volume by increasing urine output and dilating blood vessels. BNP levels are elevated in both left-sided and right- sided heart failure, as the heart is under increased pressure and volume.
C. Increased pulmonary artery wedge pressure (PAWP)
Increased pulmonary artery wedge pressure (PAWP) is not a finding of right-sided heart failure. PAWP is a measure of the pressure in the left atrium, which reflects the pressure in the pulmonary capillaries. PAWP is elevated in left-sided heart failure, as the blood backs up in the lungs due to impaired left ventricular function. PAWP is normal or low in right-sided heart failure, as the blood backs up in the systemic circulation due to impaired right ventricular function.
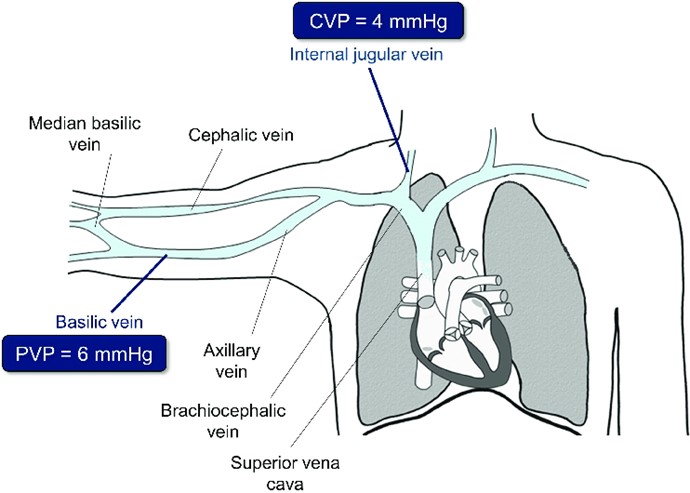
D. Elevated central venous pressure (CVP)
Elevated central venous pressure (CVP) is a finding of right-sided heart failure. CVP is a measure of the pressure in the right atrium, which reflects the pressure in the systemic venous system. CVP is elevated in right-sided heart failure, as the blood backs up in the body due to impaired right ventricular function. CVP can cause jugular venous distension, hepatomegaly, splenomegaly, ascites, and peripheral edema.
Full Explanation
Choice A: Decreased specific gravity is not a finding of right-sided heart failure. Specific gravity is a measure of urine concentration, which can be affected by fluid intake, dehydration, kidney function, and diuretic use. Right-sided heart failure does not directly affect urine concentration, but it can cause fluid retention and edema in the body.
Choice B: Decreased brain natriuretic peptide (BNP) is not a finding of right-sided heart failure. BNP is a hormone that is released by the heart when it is stretched or overloaded. BNP helps to lower blood pressure and reduce fluid volume by increasing urine output and dilating blood vessels. BNP levels are elevated in both left-sided and right- sided heart failure, as the heart is under increased pressure and volume.
Choice C: Increased pulmonary artery wedge pressure (PAWP) is not a finding of right-sided heart failure. PAWP is a measure of the pressure in the left atrium, which reflects the pressure in the pulmonary capillaries. PAWP is elevated in left-sided heart failure, as the blood backs up in the lungs due to impaired left ventricular function. PAWP is normal or low in right-sided heart failure, as the blood backs up in the systemic circulation due to impaired right ventricular function.
Choice D: Elevated central venous pressure (CVP) is a finding of right-sided heart failure. CVP is a measure of the pressure in the right atrium, which reflects the pressure in the systemic venous system. CVP is elevated in right-sided heart failure, as the blood backs up in the body due to impaired right ventricular function. CVP can cause jugular venous distension, hepatomegaly, splenomegaly, ascites, and peripheral edema.
A nurse is caring for a client who has valvular heart disease and is at risk for developing left-sided heart failure. Which of the following manifestations should alert the nurse that the client is developing this condition?
A. Weight gain
Weight gain is not a manifestation of left-sided heart failure. Weight gain is more likely to occur in right- sided heart failure, as the blood backs up in the systemic circulation and causes fluid retention and edema in the body.
B. Anorexia
Anorexia is not a manifestation of left-sided heart failure. Anorexia is a loss of appetite, which can have many causes, such as psychological disorders, infections, medications, or cancer. Left-sided heart failure does not directly affect appetite, but it can cause nausea, fatigue, and weakness.
C. Distended abdomen
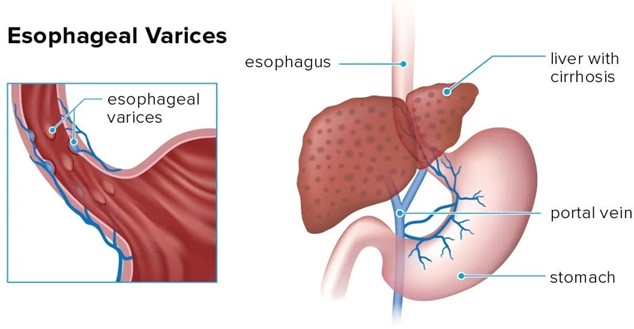
Distended abdomen is not a manifestation of left-sided heart failure. Distended abdomen is more likely to occur in right-sided heart failure, as the blood backs up in the portal vein and causes increased pressure in the liver and spleen. This can lead to hepatomegaly, splenomegaly, ascites, and varices.
D. Breathlessness
Breathlessness is a manifestation of left-sided heart failure. Breathlessness, or dyspnea, is a sensation of difficulty breathing or shortness of breath. Breathlessness occurs in left-sided heart failure, as the blood backs up in the lungs and causes pulmonary congestion and edema. This impairs gas exchange and reduces oxygen delivery to the tissues.
Full Explanation
Choice A: Weight gain is not a manifestation of left-sided heart failure. Weight gain is more likely to occur in right-sided heart failure, as the blood backs up in the systemic circulation and causes fluid retention and edema in the body.
Choice B: Anorexia is not a manifestation of left-sided heart failure. Anorexia is a loss of appetite, which can have many causes, such as psychological disorders, infections, medications, or cancer. Left-sided heart failure does not directly affect appetite, but it can cause nausea, fatigue, and weakness.
Choice C: A distended abdomen is not a manifestation of left-sided heart failure. A distended abdomen is more likely to occur in right-sided heart failure, as the blood backs up in the portal vein and causes increased pressure in the liver and spleen. This can lead to hepatomegaly, splenomegaly, ascites, and varices.
Choice D: Breathlessness is a manifestation of left-sided heart failure. Breathlessness, or dyspnea, is a sensation of difficulty breathing or shortness of breath. Breathlessness occurs in left-sided heart failure, as the blood backs up in the lungs and causes pulmonary congestion and edema. This impairs gas exchange and reduces oxygen delivery to the tissues.
A nurse is caring for a client who was admited with bleeding esophageal varices and has an esophagogastric balloon tamponade with a Sengstaken-Blakemore tube to control the bleeding. Which of the following actions should the nurse take?
A. Provide frequent oral and nares care
Provide frequent oral and nares care is the correct action for the nurse to take. Oral and nares care can help prevent infection, dryness, and irritation of the mucous membranes, which can be damaged by the pressure and friction of the tube. The nurse should also monitor the tube position, secure it with tape, and keep scissors at the bedside in case of emergency deflation.
B. Keep the client in a supine position
Keep the client in a supine position is not the correct action for the nurse to take. The supine position can increase the risk of aspiration, regurgitation, and gastric distension, which can worsen the bleeding and compromise the airway. The nurse should elevate the head of the bed to at least 30 degrees and use a semi-Fowler's or high- Fowler's position.
C. Ambulate the client four times per day
Ambulate the client four times per day is not the correct action for the nurse to take. Ambulation can increase abdominal pressure and dislodge the tube, which can cause bleeding and perforation. The nurse should keep the client on bed rest and use passive range-of-motion exercises to prevent complications such as thromboembolism and muscle atrophy.
D. Encourage the client to consume clear liquids
Encourage the client to consume clear liquids is not the correct action for the nurse to take. Clear liquids can increase gastric volume and acidity, which can aggravate the bleeding and interfere with hemostasis. The nurse should maintain nothing-by-mouth status and provide intravenous fluids and nutrition as prescribed.
Full Explanation
Choice A: Provide frequent oral and nares care is the correct action for the nurse to take. Oral and nares care can help prevent infection, dryness, and irritation of the mucous membranes, which can be damaged by the pressure and friction of the tube. The nurse should also monitor the tube position, secure it with tape, and keep scissors at the bedside in case of emergency deflation.
Choice B: Keep the client in a supine position is not the correct action for the nurse to take. The supine position can increase the risk of aspiration, regurgitation, and gastric distension, which can worsen the bleeding and compromise the airway. The nurse should elevate the head of the bed to at least 30 degrees and use a semi-Fowler's or high-Fowler's position.
Choice C: Ambulating the client four times per day is not the correct action for the nurse to take. Ambulation can increase abdominal pressure and dislodge the tube, which can cause bleeding and perforation. The nurse should keep the client on bed rest and use passive range-of-motion exercises to prevent complications such as thromboembolism and muscle atrophy.
Choice D: Encouraging the client to consume clear liquids is not the correct action for the nurse to take. Clear liquids can increase gastric volume and acidity, which can aggravate the bleeding and interfere with hemostasis. The nurse should maintain a nothing-by-mouth status and provide intravenous fluids and nutrition as prescribed.