Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
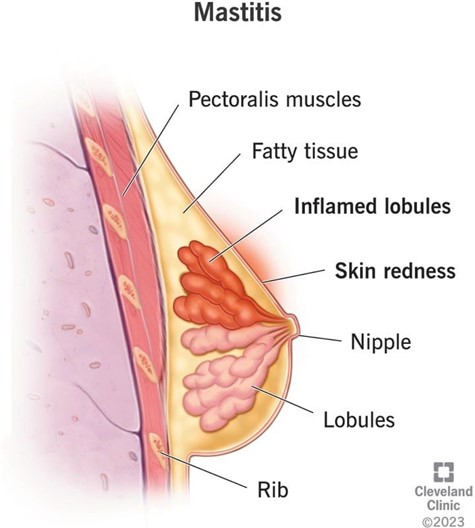
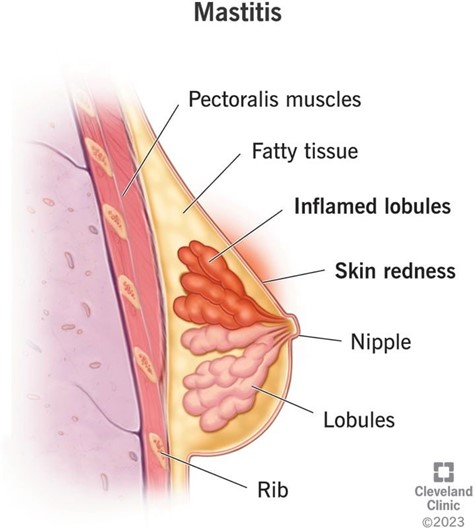
A nurse is caring for a client who is postpartum and is breastfeeding her infant. Which of the following findings indicates mastitis?
A. Swelling in both breasts
Choice A reason: Swelling in both breasts is incorrect, as this finding does not indicate mastitis. Swelling in both breasts can occur due to engorgement, which is a normal and expected phenomenon in the first few days after birth or when milk production increases. Engorgement can cause breast fullness, tenderness, and warmth, but it does not cause infection or inflammation.
B. Cracked and bleeding nipples
Choice B reason: Cracked and bleeding nipples is incorrect, as this finding does not indicate mastitis. Cracked and bleeding nipples can occur due to poor latch, improper positioning, or excessive suction of the baby. Cracked and bleeding nipples can cause pain, discomfort, and risk of infection, but they do not cause mastitis by themselves.
C. Increase in breast milk
Choice C reason: Increase in breast milk is incorrect, as this finding does not indicate mastitis. Increase in breast milk can occur due to hormonal changes, frequent breastfeeding, or stimulation of the breasts. Increase in breast milk can cause engorgement, but it does not cause infection or inflammation.
D. Red and painful area in one breast
Choice D reason: Red and painful area in one breast is correct, as this finding indicates mastitis. Mastitis is an infection and inflammation of the breast tissue that usually affects one breast at a time. Mastitis can cause redness, pain, swelling, warmth, and fever in the affected breast. Mastitis can occur due to blocked milk ducts, bacterial invasion, or poor hygiene. The nurse should advise the client to continue breastfeeding or pumping, apply warm compresses, massage the breast gently, and take antibiotics as prescribed.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Maternity Proctored Exam. Take the full exam now
Full Explanation
Choice A reason: Swelling in both breasts is incorrect, as this finding does not indicate mastitis. Swelling in both breasts can occur due to engorgement, which is a normal and expected phenomenon in the first few days after birth or when milk production increases. Engorgement can cause breast fullness, tenderness, and warmth, but it does not cause infection or inflammation.
Choice B reason: Cracked and bleeding nipples is incorrect, as this finding does not indicate mastitis. Cracked and bleeding nipples can occur due to poor latch, improper positioning, or excessive suction of the baby. Cracked and bleeding nipples can cause pain, discomfort, and risk of infection, but they do not cause mastitis by themselves.
Choice C reason: Increase in breast milk is incorrect, as this finding does not indicate mastitis. Increase in breast milk can occur due to hormonal changes, frequent breastfeeding, or stimulation of the breasts. Increase in breast milk can cause engorgement, but it does not cause infection or inflammation.
Choice D reason: Red and painful area in one breast is correct, as this finding indicates mastitis. Mastitis is an infection and inflammation of the breast tissue that usually affects one breast at a time. Mastitis can cause redness, pain, swelling, warmth, and fever in the affected breast. Mastitis can occur due to blocked milk ducts, bacterial invasion, or poor hygiene. The nurse should advise the client to continue breastfeeding or pumping, apply warm compresses, massage the breast gently, and take antibiotics as prescribed.
Similar Questions
A nurse is collecting data from a client who is 3 days postpartum and is breastfeeding. Her fundus is three fingerbreadths below the umbilicus, and her lochia rubra is moderate. Her breasts feel hard and warm. Which of the following recommendations should the nurse give the client?
A. Wear a nipple shield.
Choice A reason: Wear a nipple shield is incorrect, as this recommendation is not indicated for a client who has engorged breasts. A nipple shield is a thin, flexible device that covers the nipple and areola and can help with latch problems, flat or inverted nipples, or sore nipples. However, a nipple shield can also reduce milk transfer, stimulate less milk production, and cause nipple confusion or preference.
B. Express milk from both breasts.
Choice B reason: Express milk from both breasts is correct, as this recommendation can help relieve engorgement and maintain milk production. Engorgement is a normal and expected phenomenon that occurs when the milk comes in, usually around 72 to 96 hr after birth. Engorgement can cause breast fullness, tenderness, warmth, and hardness. The nurse should advise the client to express milk from both breasts by breastfeeding frequently and effectively or by using a breast pump or hand expression.
C. Obtain a prescription for an antibiotic.
Choice C reason: Obtain a prescription for an antibiotic is incorrect, as this recommendation is not indicated for a client who has engorged breasts. An antibiotic is used to treat mastitis, which is an infection and inflammation of the breast tissue that can cause redness, pain, swelling, warmth, and fever in the affected breast. The nurse should assess the client for signs of mastitis and report any abnormal findings to the provider.
D. Apply a heating pad to her breasts.
Choice D reason: Apply a heating pad to her breasts is incorrect, as this recommendation can worsen engorgement and cause discomfort. A heating pad can increase blood flow and swelling in the breasts, which can impair milk flow and increase pain. The nurse should advise the client to apply cold compresses or cabbage leaves to her breasts to reduce inflammation and discomfort.
Full Explanation
Choice A reason: Wear a nipple shield is incorrect, as this recommendation is not indicated for a client who has engorged breasts. A nipple shield is a thin, flexible device that covers the nipple and areola and can help with latch problems, flat or inverted nipples, or sore nipples. However, a nipple shield can also reduce milk transfer, stimulate less milk production, and cause nipple confusion or preference.
Choice B reason: Express milk from both breasts is correct, as this recommendation can help relieve engorgement and maintain milk production. Engorgement is a normal and expected phenomenon that occurs when the milk comes in, usually around 72 to 96 hr after birth. Engorgement can cause breast fullness, tenderness, warmth, and hardness. The nurse should advise the client to express milk from both breasts by breastfeeding frequently and effectively or by using a breast pump or hand expression.
Choice C reason: Obtain a prescription for an antibiotic is incorrect, as this recommendation is not indicated for a client who has engorged breasts. An antibiotic is used to treat mastitis, which is an infection and inflammation of the breast tissue that can cause redness, pain, swelling, warmth, and fever in the affected breast. The nurse should assess the client for signs of mastitis and report any abnormal findings to the provider.
Choice D reason: Apply a heating pad to her breasts is incorrect, as this recommendation can worsen engorgement and cause discomfort. A heating pad can increase blood flow and swelling in the breasts, which can impair milk flow and increase pain. The nurse should advise the client to apply cold compresses or cabbage leaves to her breasts to reduce inflammation and discomfort.
A nurse is collecting data from a client who is 24 hr postpartum. Which of the following findings should the nurse expect?
A. Fundus soft, 2 fingerbreadths below the umbilicus
Choice A reason: Fundus soft, 2 fingerbreadths below the umbilicus is incorrect, as this finding indicates uterine atony and subinvolution. The fundus is the upper part of the uterus that can be palpated through the abdomen after birth. The fundus should be firm and midline to indicate adequate uterine contraction and involution. A soft or boggy fundus can increase the risk of hemorrhage and infection.
B. Fundus firm, 1 fingerbreadth below the umbilicus
Choice B reason: Fundus firm, 1 fingerbreadth below the umbilicus is correct, as this finding indicates normal uterine contraction and involution. The fundus is normally at the level of the umbilicus immediately after birth and then descends about one fingerbreadth per day. A firm and midline fundus can prevent excessive bleeding and promote healing.
C. Fundus firm, 4 fingerbreadths above the umbilicus
Choice C reason: Fundus firm, 4 fingerbreadths above the umbilicus is incorrect, as this finding indicates a higher than expected fundal height for a client who is 24 hr postpartum. The fundus is normally at the level of the umbilicus immediately after birth and then descends about one fingerbreadth per day. A high fundal height can indicate uterine atony, retained placental fragments, or bladder distension.
D. Fundus soft, to the right of the umbilicus
Choice D reason: Fundus soft, to the right of the umbilicus is incorrect, as this finding indicates uterine atony and bladder distension. The fundus should be firm and midline to indicate adequate uterine contraction and involution. A deviated fundus can indicate bladder distension, which can interfere with uterine contraction and involution and increase the risk of hemorrhage and infection.
Full Explanation
Choice A reason: Fundus soft, 2 fingerbreadths below the umbilicus is incorrect, as this finding indicates uterine atony and subinvolution. The fundus is the upper part of the uterus that can be palpated through the abdomen after birth. The fundus should be firm and midline to indicate adequate uterine contraction and involution. A soft or boggy fundus can increase the risk of hemorrhage and infection.
Choice B reason: Fundus firm, 1 fingerbreadth below the umbilicus is correct, as this finding indicates normal uterine contraction and involution. The fundus is normally at the level of the umbilicus immediately after birth and then descends about one fingerbreadth per day. A firm and midline fundus can prevent excessive bleeding and promote healing.
Choice C reason: Fundus firm, 4 fingerbreadths above the umbilicus is incorrect, as this finding indicates a higher than expected fundal height for a client who is 24 hr postpartum. The fundus is normally at the level of the umbilicus immediately after birth and then descends about one fingerbreadth per day. A high fundal height can indicate uterine atony, retained placental fragments, or bladder distension.
Choice D reason: Fundus soft, to the right of the umbilicus is incorrect, as this finding indicates uterine atony and bladder distension. The fundus should be firm and midline to indicate adequate uterine contraction and involution. A deviated fundus can indicate bladder distension, which can interfere with uterine contraction and involution and increase the risk of hemorrhage and infection.
A nurse is assisting a client out of bed for the first time since delivery. The client becomes frightened when she passes a large amount of lochia.
Which of the following responses should the nurse make?
A. 'Lochia can pool in the vagina while you lie in bed.'
Choice A reason: This is the most appropriate response because it reassures the client that the amount of lochia she passed is normal and expected after lying down for a long time. Lochia is the vaginal discharge that occurs after childbirth, consisting of blood, mucus, and uterine tissue. It usually decreases in amount and changes in color over time, from red to pink to brown to yellow.
B. 'You might have retained fragments of your placenta.'
Choice B reason: This is an incorrect response because it implies that the client has a complication that requires further evaluation. Retained placental fragments can cause excessive bleeding, infection, and uterine atony. The nurse should not alarm the client with this possibility without evidence.
C. 'The amount of lochia increases during the postpartum period.'
Choice C reason: This is an incorrect response because it contradicts the normal patern of lochia. The amount of lochia usually decreases during the postpartum period, not increases. If the client has an increase in lochia, it could indicate a problem such as infection, subinvolution, or hemorrhage.
D. 'Urinary tract infections are associated with increased lochia.'
Choice D reason: This is an incorrect response because it confuses the client with unrelated information. Urinary tract infections are not associated with increased lochia. They are caused by bacteria entering the urinary tract and can cause symptoms such as dysuria, frequency, urgency, and hematuria. The nurse should not suggest that the client has a urinary tract infection without evidence.
Full Explanation
Choice A reason: This is the most appropriate response because it reassures the client that the amount of lochia she passed is normal and expected after lying down for a long time. Lochia is the vaginal discharge that occurs after childbirth, consisting of blood, mucus, and uterine tissue. It usually decreases in amount and changes in color over time, from red to pink to brown to yellow.
Choice B reason: This is an incorrect response because it implies that the client has a complication that requires further evaluation. Retained placental fragments can cause excessive bleeding, infection, and uterine atony. The nurse should not alarm the client with this possibility without evidence.
Choice C reason: This is an incorrect response because it contradicts the normal patern of lochia. The amount of lochia usually decreases during the postpartum period, not increases. If the client has an increase in lochia, it could indicate a problem such as infection, subinvolution, or hemorrhage.
Choice D reason: This is an incorrect response because it confuses the client with unrelated information. Urinary tract infections are not associated with increased lochia. They are caused by bacteria entering the urinary tract and can cause symptoms such as dysuria, frequency, urgency, and hematuria. The nurse should not suggest that the client has a urinary tract infection without evidence.
