Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is assisting a client out of bed for the first time since delivery. The client becomes frightened when she passes a large amount of lochia.
Which of the following responses should the nurse make?
A. 'Lochia can pool in the vagina while you lie in bed.'
Choice A reason: This is the most appropriate response because it reassures the client that the amount of lochia she passed is normal and expected after lying down for a long time. Lochia is the vaginal discharge that occurs after childbirth, consisting of blood, mucus, and uterine tissue. It usually decreases in amount and changes in color over time, from red to pink to brown to yellow.
B. 'You might have retained fragments of your placenta.'
Choice B reason: This is an incorrect response because it implies that the client has a complication that requires further evaluation. Retained placental fragments can cause excessive bleeding, infection, and uterine atony. The nurse should not alarm the client with this possibility without evidence.
C. 'The amount of lochia increases during the postpartum period.'
Choice C reason: This is an incorrect response because it contradicts the normal patern of lochia. The amount of lochia usually decreases during the postpartum period, not increases. If the client has an increase in lochia, it could indicate a problem such as infection, subinvolution, or hemorrhage.
D. 'Urinary tract infections are associated with increased lochia.'
Choice D reason: This is an incorrect response because it confuses the client with unrelated information. Urinary tract infections are not associated with increased lochia. They are caused by bacteria entering the urinary tract and can cause symptoms such as dysuria, frequency, urgency, and hematuria. The nurse should not suggest that the client has a urinary tract infection without evidence.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Maternity Proctored Exam. Take the full exam now
Full Explanation
Choice A reason: This is the most appropriate response because it reassures the client that the amount of lochia she passed is normal and expected after lying down for a long time. Lochia is the vaginal discharge that occurs after childbirth, consisting of blood, mucus, and uterine tissue. It usually decreases in amount and changes in color over time, from red to pink to brown to yellow.
Choice B reason: This is an incorrect response because it implies that the client has a complication that requires further evaluation. Retained placental fragments can cause excessive bleeding, infection, and uterine atony. The nurse should not alarm the client with this possibility without evidence.
Choice C reason: This is an incorrect response because it contradicts the normal patern of lochia. The amount of lochia usually decreases during the postpartum period, not increases. If the client has an increase in lochia, it could indicate a problem such as infection, subinvolution, or hemorrhage.
Choice D reason: This is an incorrect response because it confuses the client with unrelated information. Urinary tract infections are not associated with increased lochia. They are caused by bacteria entering the urinary tract and can cause symptoms such as dysuria, frequency, urgency, and hematuria. The nurse should not suggest that the client has a urinary tract infection without evidence.

Similar Questions
A nurse is reviewing the medical record of a client who experienced a vaginal birth 2 hours ago. The nurse should identify that which of the following findings places the client at risk for a postpartum hemorrhage?
A. Precipitous birth
Choice A reason: A precipitous birth is a delivery that occurs in less than 3 hours from the onset of labor. This can cause uterine atony, which is the failure of the uterus to contract and compress the blood vessels after the placenta is delivered. Uterine atony is the most common cause of postpartum hemorrhage²³.
B. Small for gestational age newborn
Choice B reason: A small for gestational age newborn is not a risk factor for postpartum hemorrhage. It may be associated with other conditions, such as placental insufficiency or intrauterine growth restriction, but these do not directly increase the risk of bleeding after delivery.
C. Two-vessel umbilical cord
Choice C reason: A two-vessel umbilical cord is a cord that has one artery and one vein instead of the normal two arteries and one vein. This can be a marker for congenital anomalies or placental abnormalities, but it does not increase the risk of postpartum hemorrhage by itself.
D. Gestational hypertension
Choice D reason: Gestational hypertension is a condition where the blood pressure rises above 140/90 mm Hg after 20 weeks of pregnancy. It can lead to complications such as preeclampsia, eclampsia, or HELLP syndrome, which can affect the clotting system and cause bleeding disorders. However, gestational hypertension alone does not increase the risk of postpartum hemorrhage unless it is associated with these severe conditions¹⁴.
Full Explanation
Choice A reason: A precipitous birth is a delivery that occurs in less than 3 hours from the onset of labor. This can cause uterine atony, which is the failure of the uterus to contract and compress the blood vessels after the placenta is delivered. Uterine atony is the most common cause of postpartum hemorrhage²³.
Choice B reason: A small for gestational age newborn is not a risk factor for postpartum hemorrhage. It may be associated with other conditions, such as placental insufficiency or intrauterine growth restriction, but these do not directly increase the risk of bleeding after delivery.
Choice C reason: A two-vessel umbilical cord is a cord that has one artery and one vein instead of the normal two arteries and one vein. This can be a marker for congenital anomalies or placental abnormalities, but it does not increase the risk of postpartum hemorrhage by itself.
Choice D reason: Gestational hypertension is a condition where the blood pressure rises above 140/90 mm Hg after 20 weeks of pregnancy. It can lead to complications such as preeclampsia, eclampsia, or HELLP syndrome, which can affect the clotting system and cause bleeding disorders. However, gestational hypertension alone does not increase the risk of postpartum hemorrhage unless it is associated with these severe conditions¹⁴.
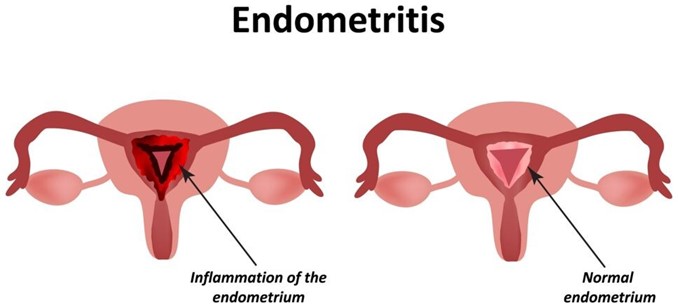
A nurse is collecting data from a client who gave birth one week ago. Which of the following findings should the nurse identify as a manifestation of endometritis?
A. Hematuria
Choice A reason: Hematuria is blood in the urine. It is not a symptom of endometritis, which is an inflammation or infection of the uterine lining. Hematuria can have many other causes, such as urinary tract infections, kidney stones, bladder cancer, or trauma.
B. Pelvic pain
Choice B reason: Pelvic pain is one of the most common symptoms of endometritis. It can be caused by the inflammation or infection of the uterine lining, which can also spread to other pelvic organs. Pelvic pain can be dull, sharp, cramping, or constant, and it may worsen with movement or intercourse¹³.
C. Pink lochia
Choice C reason: Pink lochia is normal vaginal discharge after childbirth. It consists of blood, mucus, and tissue from the uterus. It usually lasts for a few weeks and gradually changes color from red to pink to brown to white. Pink lochia is not a sign of endometritis, unless it is foul-smelling, heavy, or persists beyond six weeks.
D. Bradycardia
Choice D reason: Bradycardia is a slow heart rate, usually below 60 beats per minute. It is not a symptom of endometritis, which can cause fever and tachycardia (fast heart rate). Bradycardia can have many other causes, such as heart disease, medication side effects, hypothyroidism, or electrolyte imbalance.
Full Explanation
Choice A reason: Hematuria is blood in the urine. It is not a symptom of endometritis, which is an inflammation or infection of the uterine lining. Hematuria can have many other causes, such as urinary tract infections, kidney stones, bladder cancer, or trauma.
Choice B reason: Pelvic pain is one of the most common symptoms of endometritis. It can be caused by the inflammation or infection of the uterine lining, which can also spread to other pelvic organs. Pelvic pain can be dull, sharp, cramping, or constant, and it may worsen with movement or intercourse¹³.
Choice C reason: Pink lochia is normal vaginal discharge after childbirth. It consists of blood, mucus, and tissue from the uterus. It usually lasts for a few weeks and gradually changes color from red to pink to brown to white. Pink lochia is not a sign of endometritis, unless it is foul-smelling, heavy, or persists beyond six weeks.
Choice D reason: Bradycardia is a slow heart rate, usually below 60 beats per minute. It is not a symptom of endometritis, which can cause fever and tachycardia (fast heart rate). Bradycardia can have many other causes, such as heart disease, medication side effects, hypothyroidism, or electrolyte imbalance.
A nurse is assisting a nurse midwife in examining a client who is a primigravida at 42 weeks of gestation and states that she thinks she is in labor. Which of the following findings confirm that the client is in labor?
A. Amniotic fluid in the vaginal vault
Choice A reason: Amniotic fluid in the vaginal vault indicates that the membranes have ruptured, but this does not necessarily mean that the client is in labor. Some women may have a slow leak of amniotic fluid for hours or days before labor begins. Rupture of membranes also increases the risk of infection, so the nurse should monitor the client's temperature and fetal heart rate.
B. Contractions every 3 to 4 minutes
Choice B reason: Contractions every 3 to 4 minutes are a sign of labor, but they are not enough to confirm it. The nurse should also assess the duration and intensity of the contractions, as well as the client's response to them. Some women may have false labor contractions, also known as Braxton Hicks contractions, which are irregular, mild, and do not cause cervical changes.
C. Pain just above the navel
Choice C reason: Pain just above the navel is not a typical sign of labor. It may indicate other problems, such as placental abruption, uterine rupture, or fetal distress. The nurse should report this finding to the nurse midwife and check for other signs of bleeding, shock, or fetal compromise.
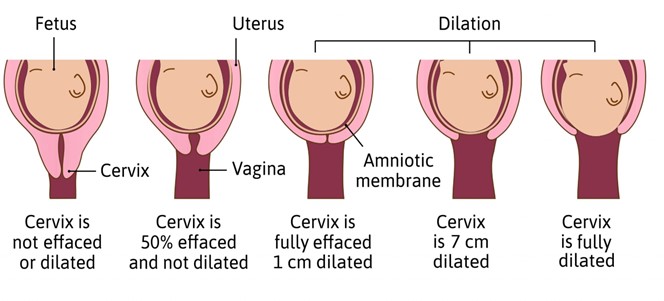
D. Cervical dilation
Choice D reason: Cervical dilation is the most reliable indicator of labor. It means that the cervix is opening and thinning out to allow the passage of the fetus. The nurse should measure the cervical dilation in centimeters and document it along with the station and effacement of the cervix.
Full Explanation
Choice A reason: Amniotic fluid in the vaginal vault indicates that the membranes have ruptured, but this does not necessarily mean that the client is in labor. Some women may have a slow leak of amniotic fluid for hours or days before labor begins. Rupture of membranes also increases the risk of infection, so the nurse should monitor the client's temperature and fetal heart rate.
Choice B reason: Contractions every 3 to 4 minutes are a sign of labor, but they are not enough to confirm it. The nurse should also assess the duration and intensity of the contractions, as well as the client's response to them. Some women may have false labor contractions, also known as Braxton Hicks contractions, which are irregular, mild, and do not cause cervical changes.
Choice C reason: Pain just above the navel is not a typical sign of labor. It may indicate other problems, such as placental abruption, uterine rupture, or fetal distress. The nurse should report this finding to the nurse midwife and check for other signs of bleeding, shock, or fetal compromise.
Choice D reason: Cervical dilation is the most reliable indicator of labor. It means that the cervix is opening and thinning out to allow the passage of the fetus. The nurse should measure the cervical dilation in centimeters and document it along with the station and effacement of the cervix.