Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is caring for a group of adolescents. Which of the following findings should be reported to the provider immediately?
A. A client who has a burn injury to an estimated 5% of his leg and is crying
A client who has a burn injury to an estimated 5% of his leg and is crying - While it's essential to assess and address the client's pain and comfort, this finding does not indicate an immediate need for medical attention. Pain management and wound care can be addressed based on the severity of the burn and the client's pain level.
B. A client who has an ankle fracture reports a pain level increase from 3 to 5 after initial ambulation
A client who has an ankle fracture reports a pain level increase from 3 to 5 after initial ambulation - This finding is concerning, and the nurse should notify the provider to reassess pain management and evaluate for potential complications related to the fracture. However, it may not require immediate medical attention unless there are signs of severe pain or complications.
C. A who is a client 1 day postoperative and has a temperature of 37.5° C (99.5° F)
A client who is 1 day postoperative and has a temperature of 37.5° C (99.5° F) - A slight increase in temperature in the immediate postoperative period may not be unusual and can be attributed to the normal inflammatory response after surgery. The nurse should continue monitoring the client's temperature and report any further changes or additional signs of infection or complications to the provider.Overall, while all findings should be addressed and managed appropriately, the significant drop in blood pressure (option D) should be reported immediately due to the potential implications for the client's overall health and well-being.
D. A client's blood pressure changes from 112/60 mm Hg to 90/54 mm Hg when standing
A client's blood pressure changes from 112/60 mm Hg to 90/54 mm Hg when standing. A significant drop in blood pressure when changing positions from lying to standing may indicate orthostatic hypotension, which can be a sign of dehydration, blood loss, or other underlying medical issues. This can be a cause for concern, especially if the client is an a
This question is an excerpt from Nurse Dive's nursing test bank - SIMMONS U BSN PEDIATRICS PROCTORED EXAM. Take the full exam now
Full Explanation
D. A client's blood pressure changes from 112/60 mm Hg to 90/54 mm Hg when standing.
A significant drop in blood pressure when changing positions from lying to standing may indicate orthostatic hypotension, which can be a sign of dehydration, blood loss, or other underlying medical issues. This can be a cause for concern, especially if the client is an adolescent, as it may lead to decreased perfusion of vital organs and may require immediate medical attention.
The other options are as follows:
A. A client who has a burn injury to an estimated 5% of his leg and is crying - While it's essential to assess and address the client's pain and comfort, this finding does not indicate an immediate need for medical attention. Pain management and wound care can be addressed based on the severity of the burn and the client's pain level.
B. A client who has an ankle fracture reports a pain level increase from 3 to 5 after initial ambulation - This finding is concerning, and the nurse should notify the provider to reassess pain management and evaluate for potential complications related to the fracture. However, it may not require immediate medical attention unless there are signs of severe pain or complications.
C. A client who is 1 day postoperative and has a temperature of 37.5° C (99.5° F) - A slight increase in temperature in the immediate postoperative period may not be unusual and can be attributed to the normal inflammatory response after surgery. The nurse should continue monitoring the client's temperature and report any further changes or additional signs of infection or complications to the provider.
Overall, while all findings should be addressed and managed appropriately, the significant drop in blood pressure (option D) should be reported immediately due to the potential implications for the client's overall health and well-being.
Similar Questions
A nurse is caring for an infant who has a congenital heart defect. Which of the following defects is associated with increased pulmonary blood flow?
A. Coarctation of the aorta
Coarctation of the aorta - Coarctation of the aorta is a narrowing of the aorta, which obstructs blood flow and leads to increased blood pressure in the upper body and reduced blood flow to the lower body.
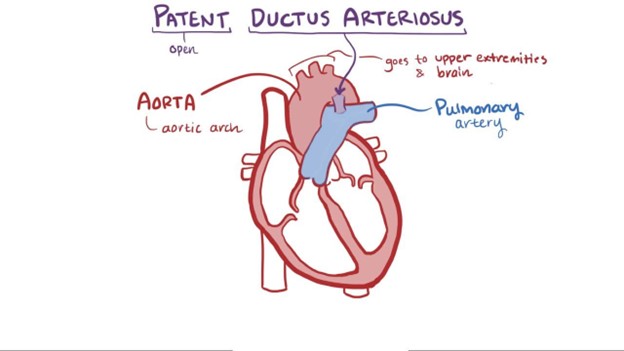
B. Patent ductus arteriosus
A patent ductus arteriosus (PDA) is a congenital heart defect associated with increased pulmonary blood flow. In normal fetal circulation, the ductus arteriosus allows blood to bypass the lungs since the baby receives oxygen from the mother's placenta. After birth, the ductus arteriosus should close, redirecting blood flow to the lungs for oxygenation. However, in some infants with PDA, the ductus arteriosus remains open, causing an abnormal connection between the aorta and the pulmonary artery. As a result, oxygenated blood from the aorta flows back into the pulmonary artery, increasing the workload on the lungs.
C. Tetralogy of Fallot
Tetralogy of Fallot - Tetralogy of Fallot is a combination of four heart defects that results in decreased pulmonary blood flow due to a ventricular septal defect (VSD), overriding aorta, pulmonary stenosis, and right ventricular hypertrophy.
D. Tricuspid atresia
Tricuspid atresia - Tricuspid atresia is a congenital heart defect where the tricuspid valve does not develop correctly, resulting in an absent or abnormal tricuspid valve. This defect prevents blood flow from the right atrium to the right ventricle and, therefore, reduces pulmonary blood flow.
Full Explanation
A patent ductus arteriosus (PDA) is a congenital heart defect associated with increased pulmonary blood flow. In normal fetal circulation, the ductus arteriosus allows blood to bypass the lungs since the baby receives oxygen from the mother's placenta. After birth, the ductus arteriosus should close, redirecting blood flow to the lungs for oxygenation. However, in some infants with PDA, the ductus arteriosus remains open, causing an abnormal connection between the aorta and the pulmonary artery. As a result, oxygenated blood from the aorta flows back into the pulmonary artery, increasing the workload on the lungs.
The other options are as follows:
A. Coarctation of the aorta - Coarctation of the aorta is a narrowing of the aorta, which obstructs blood flow and leads to increased blood pressure in the upper body and reduced blood flow to the lower body.
C. Tetralogy of Fallot - Tetralogy of Fallot is a combination of four heart defects that results in decreased pulmonary blood flow due to a ventricular septal defect (VSD), overriding aorta, pulmonary stenosis, and right ventricular hypertrophy.
D. Tricuspid atresia - Tricuspid atresia is a congenital heart defect where the tricuspid valve does not develop correctly, resulting in an absent or abnormal tricuspid valve. This defect prevents blood flow from the right atrium to the right ventricle and, therefore, reduces pulmonary blood flow.
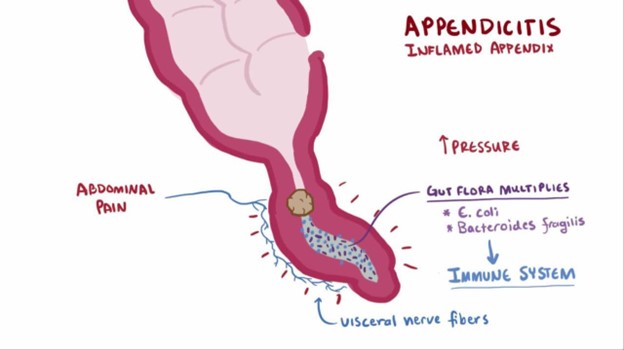
A nurse is caring for a child who has suspected appendicitis. Which of the following provider prescriptions should the nurse clarify?
A. Monitor oral temperature every 4 hr.
Monitoring oral temperature every 4 hours is important to assess for signs of infection or worsening condition.
B. Administer sodium biphosphate/sodium phosphate.
The nurse should clarify the prescription to administer sodium biphosphate/sodium phosphate because it is a laxative and is contraindicated in a child with suspected appendicitis. The use of laxatives or enemas can potentially worsen the condition by increasing the risk of perforation or rupture of the inflamed appendix.
C. Maintain NPO status.
Maintaining NPO status is essential to avoid stimulating the digestive system and to prepare for possible surgery.
D. Medicate the client for pain every 4 hr as needed.
Medicating the client for pain every 4 hours as needed is appropriate to manage pain and provide comfort while the child awaits further evaluation or treatment.Remember, it's crucial to avoid the use of laxatives, enemas, or any other interventions that can potentially aggravate the inflamed appendix in a child with suspected appendicitis.
Full Explanation
The nurse should clarify the prescription to administer sodium biphosphate/sodium phosphate because it is a laxative and is contraindicated in a child with suspected appendicitis. The use of laxatives or enemas can potentially worsen the condition by increasing the risk of perforation or rupture of the inflamed appendix.
A. Monitoring oral temperature every 4 hours is important to assess for signs of infection or worsening condition.
C. Maintaining NPO status is essential to avoid stimulating the digestive system and to prepare for possible surgery.
D. Medicating the client for pain every 4 hours as needed is appropriate to manage pain and provide comfort while the child awaits further evaluation or treatment.
Remember, it's crucial to avoid the use of laxatives, enemas, or any other interventions that can potentially aggravate the inflamed appendix in a child with suspected appendicitis.
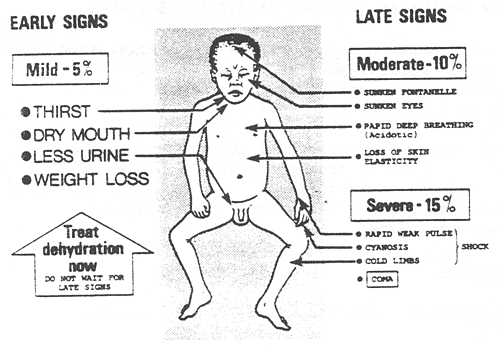
A nurse in an emergency department is assessing an infant who is dehydrated. Which of the following findings should the nurse expect?
A. Irritability
The nurse should expect to find irritability in an infant who is dehydrated. Dehydration in infants can lead to changes in behavior and irritability due to the imbalance in fluid and electrolytes. Other common signs of dehydration in infants may include: Poor skin turgor (skin tenting) Sunken fontanelles (soft spots on the baby's head) Dry mucous membranes (dry mouth and tongue) Decreased urine output or concentrated urine Rapid heart rate (tachycardia) Increased respiratory rate Sunken eyes Decreased tears when crying
B. Tetany
Tetany is a condition characterized by involuntary muscle contractions and is more commonly associated with hypocalcemia (low calcium levels) rather than dehydration.
C. slow, bounding pulse
A slow, bounding pulse is not typically associated with dehydration. Dehydration often leads to a rapid heart rate (tachycardia) as the body attempts to compensate for the loss of fluid.
D. Decreased temperature
Decreased temperature is not a typical finding in dehydration. Dehydration can lead to fever in some cases due to an underlying infection, but it does not cause a decrease in body temperature on its own.
Full Explanation
The nurse should expect to find irritability in an infant who is dehydrated. Dehydration in infants can lead to changes in behavior and irritability due to the imbalance in fluid and electrolytes. Other common signs of dehydration in infants may include:
Poor skin turgor (skin tenting)
Sunken fontanelles (soft spots on the baby's head)
Dry mucous membranes (dry mouth and tongue)
Decreased urine output or concentrated urine
Rapid heart rate (tachycardia)
Increased respiratory rate
Sunken eyes
Decreased tears when crying
B. Tetany is a condition characterized by involuntary muscle contractions and is more commonly associated with hypocalcemia (low calcium levels) rather than dehydration.
C. A slow, bounding pulse is not typically associated with dehydration. Dehydration often leads to a rapid heart rate (tachycardia) as the body attempts to compensate for the loss of fluid.
D. Decreased temperature is not a typical finding in dehydration. Dehydration can lead to fever in some cases due to an underlying infection, but it does not cause a decrease in body temperature on its own.