Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is caring for a group of clients on an intrapartum unit. Which of the following findings should be reported to the RN immediately?
A. A client who is at 32 weeks of gestation and is experiencing irregular, frequent contractions is tearful
Choice A reason: A client who is at 32 weeks of gestation and is experiencing irregular, frequent contractions is tearful may have preterm labor, which should be monitored and treated accordingly. However, this is not as urgent as choice D, as the contractions may subside with hydration, rest, or tocolytic medication.
B. A client who has preeclampsia has 2+ patellar reflexes and 2+ proteinuria
Choice B reason: A client who has preeclampsia has 2+ patellar reflexes and 2+ proteinuria may have mild preeclampsia, which should be managed with antihypertensive medication, bed rest, and fetal monitoring. However, this is not as urgent as choice D, as the reflexes and proteinuria are not indicative of severe preeclampsia or eclampsia.
C. A client who is at 28 weeks of gestation and receiving terbutaline reports fine tremors
Choice C reason: A client who is at 28 weeks of gestation and receiving terbutaline reports fine tremors may have a common side effect of terbutaline, which is a beta-adrenergic agonist that relaxes uterine smooth muscle and inhibits contractions. However, this is not as urgent as choice D, as the tremors are usually transient and benign. The nurse should monitor the client's vital signs, blood glucose, and fetal heart rate.
D. A client who has preeclampsia and reports epigastric pain and unresolved headache
Choice D reason: A client who has preeclampsia and reports epigastric pain and unresolved headache should be reported to the RN immediately, as these are signs of severe preeclampsia and impending eclampsia, which can lead to seizures, coma, and death. The client may need anticonvulsant medication, magnesium sulfate infusion, and delivery of the fetus.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Maternity Proctored Exam. Take the full exam now
Full Explanation
Choice D reason: A client who has preeclampsia and reports epigastric pain and unresolved headache should be reported to the RN immediately, as these are signs of severe preeclampsia and impending eclampsia, which can lead to seizures, coma, and death. The client may need anticonvulsant medication, magnesium sulfate infusion, and delivery of the fetus.
Choice A reason: A client who is at 32 weeks of gestation and is experiencing irregular, frequent contractions is tearful may have preterm labor, which should be monitored and treated accordingly. However, this is not as urgent as choice D, as the contractions may subside with hydration, rest, or tocolytic medication.
Choice B reason: A client who has preeclampsia has 2+ patellar reflexes and 2+ proteinuria may have mild preeclampsia, which should be managed with antihypertensive medication, bed rest, and fetal monitoring. However, this is not as urgent as choice D, as the reflexes and proteinuria are not indicative of severe preeclampsia or eclampsia.
Choice C reason: A client who is at 28 weeks of gestation and receiving terbutaline reports fine tremors may have a common side effect of terbutaline, which is a beta-adrenergic agonist that relaxes uterine smooth muscle and inhibits contractions. However, this is not as urgent as choice D, as the tremors are usually transient and benign. The nurse should monitor the client's vital signs, blood glucose, and fetal heart rate.
Similar Questions
A nurse is collecting data from a postpartum client and finds a large amount of lochia rubra with several clots on the client's perineal pad. Which of the following actions should the nurse take first?
A. Feel for a full bladder.
Choice A reason: Feeling for a full bladder is not the first action the nurse should take, although it is important to assess for bladder distension and urinary retention in postpartum clients. A full bladder can displace the uterus and increase the risk of uterine atony and hemorrhage.
B. Check the client's fundus.
Choice B reason: Checking the client's fundus is the first action the nurse should take, as it can indicate the tone and position of the uterus. A firm and midline fundus indicates adequate uterine contraction and prevents excessive bleeding. A boggy or deviated fundus indicates uterine atony or retained placental fragments, which can cause hemorrhage.
C. Measure the client's vital signs.
Choice C reason: Measuring the client's vital signs is not the first action the nurse should take, although it is important to monitor for signs of shock and infection in postpartum clients. Vital signs can be affected by various factors and do not provide a direct assessment of uterine status.
D. Request the provider perform a vaginal examination.
Choice D reason: Requesting the provider perform a vaginal examination is not the first action the nurse should take, as it can introduce infection and trauma to the perineum. A vaginal examination is only indicated if there is suspicion of cervical or vaginal lacerations or retained placenta.
Full Explanation
Choice A reason:
Feeling for a full bladder is not the first action the nurse should take, although it is important to assess for bladder distension and urinary retention in postpartum clients. A full bladder can displace the uterus and increase the risk of uterine atony and hemorrhage.
Choice B reason:
Checking the client's fundus is the first action the nurse should take, as it can indicate the tone and position of the uterus. A firm and midline fundus indicates adequate uterine contraction and prevents excessive bleeding. A boggy or deviated fundus indicates uterine atony or retained placental fragments, which can cause hemorrhage.
Choice C reason:
Measuring the client's vital signs is not the first action the nurse should take, although it is important to monitor for signs of shock and infection in postpartum clients. Vital signs can be affected by various factors and do not provide a direct assessment of uterine status.
Choice D reason:
Requesting the provider perform a vaginal examination is not the first action the nurse should take, as it can introduce infection and trauma to the perineum. A vaginal examination is only indicated if there is suspicion of cervical or vaginal lacerations or retained placenta.
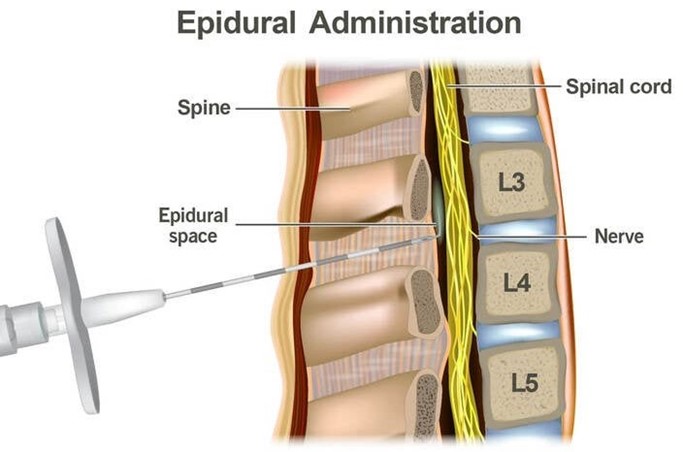
A nurse is reinforcing teaching with a client who is in labor about why epidural anesthesia is not initiated until a good labor patern has been established. Which of the following explanations should the nurse include?
A. "Given too soon, epidural anesthesia can cause fetal depression."
Choice A reason: Given too soon, epidural anesthesia can cause fetal depression is incorrect, as epidural anesthesia does not cross the placenta and does not affect the fetal status.
B. "Given too soon, epidural anesthesia will delay rupture of fetal membranes."
Choice B reason: Given too soon, epidural anesthesia will delay rupture of fetal membranes is incorrect, as epidural anesthesia does not interfere with the rupture of membranes. The rupture of membranes depends on the cervical dilation and effacement, the position of the presenting part, and the strength of contractions.
C. "Given too soon, epidural anesthesia can cause maternal hypertension."
Choice C reason: Given too soon, epidural anesthesia can cause maternal hypertension is incorrect, as epidural anesthesia can cause maternal hypotension due to vasodilation and decreased venous return. The nurse should monitor the client's blood pressure and administer fluids and vasopressors as needed.
D. "Given too soon, epidural anesthesia can prolong labor."
Choice D reason: Given too soon, epidural anesthesia can prolong labor is correct, as epidural anesthesia can decrease the strength and frequency of contractions and reduce the urge to push. The nurse should ensure that the client has a good labor patern before administering epidural anesthesia and monitor the progress of labor afterwards.
Full Explanation
Choice A reason:
Given too soon, epidural anesthesia can cause fetal depression is incorrect, as epidural anesthesia does not cross the placenta and does not affect the fetal status.
Choice B reason:
Given too soon, epidural anesthesia will delay rupture of fetal membranes is incorrect, as epidural anesthesia does not interfere with the rupture of membranes. The rupture of membranes depends on the cervical dilation and effacement, the position of the presenting part, and the strength of contractions.
Choice C reason:
Given too soon, epidural anesthesia can cause maternal hypertension is incorrect, as epidural anesthesia can cause maternal hypotension due to vasodilation and decreased venous return. The nurse should monitor the client's blood pressure and administer fluids and vasopressors as needed.
Choice D reason:
Given too soon, epidural anesthesia can prolong labor is correct, as epidural anesthesia can decrease the strength and frequency of contractions and reduce the urge to push. The nurse should ensure that the client has a good labor patern before administering epidural anesthesia and monitor the progress of labor afterwards.
A nurse is assisting with the care of a client who is in labor. The client's labor is difficult and prolonged and she reports a severe backache. Which of the following factors is a contributing cause of difficult, prolonged labor?
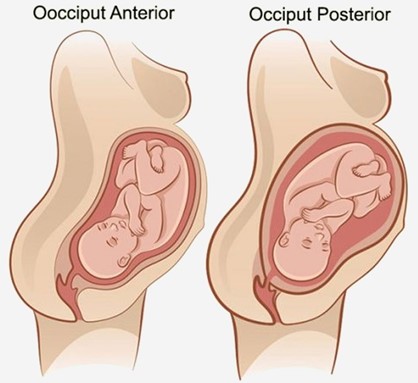
A. Fetal position is persistent occiput posterior.
Choice A reason: Fetal position is persistent occiput posterior is correct, as this position can cause difficult, prolonged labor and severe backache. The occiput posterior position means that the back of the fetal head is facing the maternal sacrum, which can result in poor alignment and descent, increased pressure on the maternal sacrum and nerves, and increased risk of perineal trauma. The nurse should encourage the client to change positions frequently, use pelvic rocking exercises, apply counterpressure to the sacrum, and administer analgesics as needed.
B. Fetal attitude is in general flexion.
Choice B reason: Fetal attitude is in general flexion is incorrect, as this attitude can facilitate normal labor and delivery. The fetal attitude refers to the degree of flexion or extension of the fetal head and limbs in relation to the fetal trunk. General flexion means that the fetal head is flexed on the chest, the arms are crossed over the chest, and the legs are flexed at the knees. This attitude allows the smallest diameter of the fetal head to pass through the birth canal.
C. Fetal lie is longitudinal.
Choice C reason: Fetal lie is longitudinal is incorrect, as this lie can facilitate normal labor and delivery. The fetal lie refers to the relationship between the long axis of the fetus and the long axis of the mother. Longitudinal lie means that both axes are parallel, which allows for either a vertex (head-first) or a breech (butocks-first) presentation.
D. Maternal pelvis is gynecoid.
Choice D reason: Maternal pelvis is gynecoid is incorrect, as this pelvis can facilitate normal labor and delivery. The maternal pelvis refers to the shape and size of the bony pelvis that affects the passage of the fetus. Gynecoid pelvis is the most common and favorable type for vaginal birth, as it has a rounded inlet, a wide pubic arch, and adequate outlet dimensions.
Full Explanation
Choice A reason:
Fetal position is persistent occiput posterior is correct, as this position can cause difficult, prolonged labor and severe backache. The occiput posterior position means that the back of the fetal head is facing the maternal sacrum, which can result in poor alignment and descent, increased pressure on the maternal sacrum and nerves, and increased risk of perineal trauma. The nurse should encourage the client to change positions frequently, use pelvic rocking exercises, apply counterpressure to the sacrum, and administer analgesics as needed.
Choice B reason:
Fetal attitude is in general flexion is incorrect, as this attitude can facilitate normal labor and delivery. The fetal attitude refers to the degree of flexion or extension of the fetal head and limbs in relation to the fetal trunk. General flexion means that the fetal head is flexed on the chest, the arms are crossed over the chest, and the legs are flexed at the knees. This attitude allows the smallest diameter of the fetal head to pass through the birth canal.
Choice C reason:
Fetal lie is longitudinal is incorrect, as this lie can facilitate normal labor and delivery. The fetal lie refers to the relationship between the long axis of the fetus and the long axis of the mother. Longitudinal lie means that both axes are parallel, which allows for either a vertex (head-first) or a breech (butocks-first) presentation.
Choice D reason:
Maternal pelvis is gynecoid is incorrect, as this pelvis can facilitate normal labor and delivery. The maternal pelvis refers to the shape and size of the bony pelvis that affects the passage of the fetus. Gynecoid pelvis is the most common and favorable type for vaginal birth, as it has a rounded inlet, a wide pubic arch, and adequate outlet dimensions.