Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
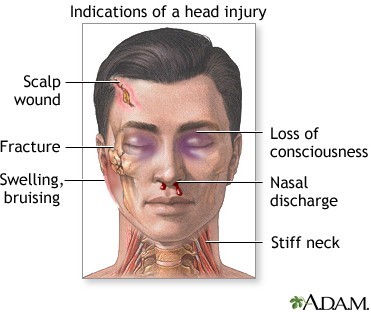
A nurse is collecting data from a client who has a traumatic head injury. Which of the following findings should the nurse report to the provider immediately?
A. Sudden sleepiness
The nurse should report sudden sleepiness to the provider immediately if the client has a traumatic head injury. Sudden sleepiness can indicate an increase in intracranial pressure, which can be a life-threatening complication of a head injury. Headache, diplopia, and slight ataxia are also important findings that the nurse should report to the provider. However, these findings are not as urgent as sudden sleepiness. Headache can be a common symptom following a head injury. Diplopia is double vision and can indicate cranial nerve damage. Slight ataxia is unsteadiness or lack of coordination and can indicate neurological damage.
B. Headache
C. Diplopia
D. Slight ataxia
This question is an excerpt from Nurse Dive's nursing test bank - ATI Custom MS Nurse Proctored Exam. Take the full exam now
Full Explanation
The nurse should report sudden sleepiness to the provider immediately if the client has a traumatic head injury. Sudden sleepiness can indicate an increase in intracranial pressure, which can be a life-threatening complication of a head injury.
Headache, diplopia, and slight ataxia are also important findings that the nurse should report to the provider. However, these findings are not as urgent as sudden sleepiness. Headache can be a common symptom following a head injury. Diplopia is double vision and can indicate cranial nerve damage. Slight ataxia is unsteadiness or lack of coordination and can indicate neurological damage.
Similar Questions
A nurse is collecting data from a client who has a score of 8 using the Glasgow Coma Scale. Which of the following findings should the nurse expect?
A. The client requires total nursing care.
A GCS score of 8 indicates severe impairment, suggesting the client may be in a state where they cannot perform basic self-care activities and thus require total nursing care.
B. The client is in a deep coma.
A GCS score of 8 indicates severe impairment but not necessarily a deep coma. Scores below 8 suggest a comatose state, but deep coma is more likely to be indicated by a score of 3-4.
C. The client is alert and oriented.
A GCS score of 8 is not consistent with a client who is alert and oriented. This score indicates significant neurological impairment.
D. The client has a stable neurological status.
A GCS score of 8 does not indicate stable neurological status. It suggests severe impairment and potentially unstable or deteriorating neurological condition.
Full Explanation
a. A GCS score of 8 indicates severe impairment, suggesting the client may be in a state where they cannot perform basic self-care activities and thus require total nursing care.
b. A GCS score of 8 indicates severe impairment but not necessarily a deep coma. Scores below 8 suggest a comatose state, but deep coma is more likely to be indicated by a score of 3-4.
c. A GCS score of 8 is not consistent with a client who is alert and oriented. This score indicates significant neurological impairment.
d. A GCS score of 8 does not indicate stable neurological status. It suggests severe impairment and potentially unstable or deteriorating neurological condition.
A nurse is caring for a client who is 2 days postoperative following an above-the-knee amputation. Which of the following is an appropriate nursing intervention for the client at this time?
A. Elevate the foot of the bed.
B. Encourage sitting up as much as possible.
C. Elevate the stump on a pillow.
D. Have the client lie prone several times each day.
Having the client lie prone several times each day is an appropriate nursing intervention for a client who is 2 days postoperative following an above-the-knee amputation. Lying prone can help prevent hip flexion contractures, which can occur after an above-the-knee amputation². a. Elevating the foot of the bed is not an appropriate intervention for a client who is 2 days postoperative following an above-the-knee amputation. b. Encouraging sitting up as much as possible is not an appropriate intervention for a client who is 2 days postoperative following an above-the-knee amputation. c. Elevating the stump on a pillow is not an appropriate intervention for a client who is 2 days postoperative following an above-the-knee amputation.
Full Explanation
Having the client lie prone several times each day is an appropriate nursing intervention for a client who is 2 days postoperative following an above-the-knee amputation. Lying prone can help prevent hip flexion contractures, which can occur after an above-the-knee amputation².
a. Elevating the foot of the bed is not an appropriate intervention for a client who is 2 days postoperative following an above-the-knee amputation.
b. Encouraging sitting up as much as possible is not an appropriate intervention for a client who is 2 days postoperative following an above-the-knee amputation.
c. Elevating the stump on a pillow is not an appropriate intervention for a client who is 2 days postoperative following an above-the-knee amputation.
A nurse is caring for a client who sustained a basal skull fracture. When performing morning hygiene care, the nurse notices a thin stream of clear drainage coming from out of the client's right nostril. Which of the following actions should the nurse take first?
A. Test the drainage for glucose.
The first action the nurse should take is to test the drainage for glucose. Clear drainage from the nose following a basal skull fracture could indicate a cerebrospinal fluid (CSF) leak. CSF contains glucose, so testing the drainage for glucose can help determine if it is CSF.
B. Take the client's temperature.
Taking the client's temperature is not the first action the nurse should take.
C. Notify the charge nurse.
Notifying the charge nurse is important but not the first action the nurse should take.
D. Place a dressing under the client's nose.
Placing a dressing under the client's nose is not the first action the nurse should take.
Full Explanation
The first action the nurse should take is to test the drainage for glucose. Clear drainage from the nose following a basal skull fracture could indicate a cerebrospinal fluid (CSF) leak. CSF contains glucose, so testing the drainage for glucose can help determine if it is CSF.
b. Taking the client's temperature is not the first action the nurse should take.
c. Notifying the charge nurse is important but not the first action the nurse should take.
d. Placing a dressing under the client's nose is not the first action the nurse should take.