Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is collecting data from a postpartum client and notes the client's fundus is boggy and displaced to the right. Which of the following actions should the nurse take?
A. Position the client on her left side.
Choice A reason: Position the client on her left side is incorrect, as this action is not indicated for a client who has a boggy and displaced fundus. Positioning the client on her left side can enhance uterine blood flow and placental perfusion, but it does not address the cause of uterine atony or bladder distension.
B. Encourage the client to perform Kegel exercises.
Choice B reason: Encourage the client to perform Kegel exercises is incorrect, as this action is not indicated for a client who has a boggy and displaced fundus. Kegel exercises can strengthen the pelvic floor muscles and prevent urinary incontinence, but they do not affect the uterine tone or position.
C. Ask the client to rate her pain.
Choice C reason: Ask the client to rate her pain is incorrect, as this action is not a priority for a client who has a boggy and displaced fundus. Asking the client to rate her pain can provide information about the need for analgesics, but it does not address the risk of hemorrhage or infection due to uterine atony or bladder distension.
D. Assist the client to the bathroom to void.
Choice D reason: Assist the client to the bathroom to void is correct, as this action can resolve the problem of a boggy and displaced fundus. A boggy and displaced fundus indicates uterine atony and bladder distension, which can interfere with uterine contraction and involution and increase the risk of hemorrhage and infection. The nurse should assist the client to empty their bladder and then massage the fundus until it becomes firm and midline.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Maternity Proctored Exam. Take the full exam now
Full Explanation
Choice A reason: Position the client on her left side is incorrect, as this action is not indicated for a client who has a boggy and displaced fundus. Positioning the client on her left side can enhance uterine blood flow and placental perfusion, but it does not address the cause of uterine atony or bladder distension.
Choice B reason: Encourage the client to perform Kegel exercises is incorrect, as this action is not indicated for a client who has a boggy and displaced fundus. Kegel exercises can strengthen the pelvic floor muscles and prevent urinary incontinence, but they do not affect the uterine tone or position.
Choice C reason: Ask the client to rate her pain is incorrect, as this action is not a priority for a client who has a boggy and displaced fundus. Asking the client to rate her pain can provide information about the need for analgesics, but it does not address the risk of hemorrhage or infection due to uterine atony or bladder distension.
Choice D reason: Assist the client to the bathroom to void is correct, as this action can resolve the problem of a boggy and displaced fundus. A boggy and displaced fundus indicates uterine atony and bladder distension, which can interfere with uterine contraction and involution and increase the risk of hemorrhage and infection. The nurse should assist the client to empty their bladder and then massage the fundus until it becomes firm and midline.
Similar Questions
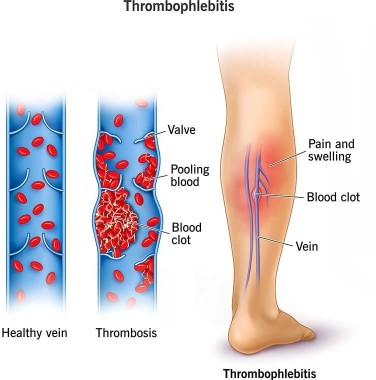
A nurse is caring for a client who is 1 day postpartum following a cesarean birth. To prevent thrombophlebitis, the nurse should contribute which of the following interventions to the client's plan of care?
A. Apply warm, moist soaks to the client's lower legs.
Choice A reason: Apply warm, moist soaks to the client's lower legs is incorrect, as this action is not effective for preventing thrombophlebitis. Warm, moist soaks can provide comfort and reduce inflammation, but they do not improve blood circulation or prevent clot formation.
B. Have the client ambulate frequently in the hallway.
Choice B reason: Have the client ambulate frequently in the hallway is correct, as this action can prevent thrombophlebitis by improving venous return and preventing stasis. The nurse should encourage and assist the client to ambulate early and frequently after a cesarean birth, as long as there are no contraindications. The nurse should also monitor the client for signs of orthostatic hypotension and provide support as needed.
C. Keep the client on bed rest.
Choice C reason: Keep the client on bed rest is incorrect, as this action can increase the risk of thrombophlebitis by reducing blood flow and promoting stasis. Bed rest can also delay wound healing and increase the risk of infection and deconditioning. The nurse should avoid keeping the client on bed rest unless absolutely necessary.
D. Place pillows under the client's knees while she is resting in bed.
Choice D reason: Place pillows under the client's knees while she is resting in bed is incorrect, as this action can impair blood circulation and increase the risk of thrombophlebitis. Placing pillows under the knees can cause pressure on the popliteal veins and reduce venous return. The nurse should advise the client to avoid crossing their legs or placing pillows under their knees while resting in bed.
Full Explanation
Choice A reason: Apply warm, moist soaks to the client's lower legs is incorrect, as this action is not effective for preventing thrombophlebitis. Warm, moist soaks can provide comfort and reduce inflammation, but they do not improve blood circulation or prevent clot formation.
Choice B reason: Have the client ambulate frequently in the hallway is correct, as this action can prevent thrombophlebitis by improving venous return and preventing stasis. The nurse should encourage and assist the client to ambulate early and frequently after a cesarean birth, as long as there are no contraindications. The nurse should also monitor the client for signs of orthostatic hypotension and provide support as needed.
Choice C reason: Keep the client on bed rest is incorrect, as this action can increase the risk of thrombophlebitis by reducing blood flow and promoting stasis. Bed rest can also delay wound healing and increase the risk of infection and deconditioning. The nurse should avoid keeping the client on bed rest unless absolutely necessary.
Choice D reason: Place pillows under the client's knees while she is resting in bed is incorrect, as this action can impair blood circulation and increase the risk of thrombophlebitis. Placing pillows under the knees can cause pressure on the popliteal veins and reduce venous return. The nurse should advise the client to avoid crossing their legs or placing pillows under their knees while resting in bed.
A nurse is caring for a client who is postpartum. Which of the following findings is an indication for the nurse to administer Rho(D) immune globulin?
A. The client is Rh negative and the newborn is Rh positive.
Choice A reason: The client is Rh negative and the newborn is Rh positive is correct, as this finding indicates a risk of Rh incompatibility and sensitization. Rh incompatibility occurs when the mother has Rh-negative blood and the baby has Rh-positive blood, which can cause maternal antibodies to atack the fetal red blood cells. Sensitization occurs when the maternal antibodies cross the placenta and enter the fetal circulation, which can cause hemolytic disease of the newborn. The nurse should administer Rho(D) immune globulin to prevent sensitization and protect future pregnancies.
B. The client is Rh negative and the newborn is Rh negative.
Choice B reason: The client is Rh negative and the newborn is Rh negative is incorrect, as this finding does not indicate a risk of Rh incompatibility or sensitization. If both the mother and the baby have Rh-negative blood, there is no antigen-antibody reaction and no need for Rho(D) immune globulin.
C. The client is Rh positive and the newborn is Rh positive.
Choice C reason: The client is Rh positive and the newborn is Rh positive is incorrect, as this finding does not indicate a risk of Rh incompatibility or sensitization. If both the mother and the baby have Rh-positive blood, there is no antigen-antibody reaction and no need for Rho(D) immune globulin.
D. The client is Rh positive and the newborn is Rh negative.
Choice D reason: The client is Rh positive and the newborn is Rh negative is incorrect, as this finding does not indicate a risk of Rh incompatibility or sensitization. If the mother has Rh-positive blood and the baby has Rh- negative blood, there is no antigen-antibody reaction and no need for Rho(D) immune globulin.
Full Explanation
Choice A reason: The client is Rh negative and the newborn is Rh positive is correct, as this finding indicates a risk of Rh incompatibility and sensitization. Rh incompatibility occurs when the mother has Rh-negative blood and the baby has Rh-positive blood, which can cause maternal antibodies to atack the fetal red blood cells. Sensitization occurs when the maternal antibodies cross the placenta and enter the fetal circulation, which can cause hemolytic disease of the newborn. The nurse should administer Rho(D) immune globulin to prevent sensitization and protect future pregnancies.
Choice B reason: The client is Rh negative and the newborn is Rh negative is incorrect, as this finding does not indicate a risk of Rh incompatibility or sensitization. If both the mother and the baby have Rh-negative blood, there is no antigen-antibody reaction and no need for Rho(D) immune globulin.
Choice C reason: The client is Rh positive and the newborn is Rh positive is incorrect, as this finding does not indicate a risk of Rh incompatibility or sensitization. If both the mother and the baby have Rh-positive blood, there is no antigen-antibody reaction and no need for Rho(D) immune globulin.
Choice D reason: The client is Rh positive and the newborn is Rh negative is incorrect, as this finding does not indicate a risk of Rh incompatibility or sensitization. If the mother has Rh-positive blood and the baby has Rh- negative blood, there is no antigen-antibody reaction and no need for Rho(D) immune globulin.
A nurse is assisting in the care of a client who is in active labor. The nurse notes late decelerations on the fetal monitor tracing. Which of the following actions should the nurse take first?
A. Position the client on her side.
Choice A reason: Position the client on her side is correct, as this is the first action the nurse should take according to the ABCDE priority framework. Late decelerations are symmetrical decreases in the fetal heart rate that begin after the peak of the contraction and return to baseline after the contraction ends, which indicate uteroplacental insufficiency and fetal hypoxia. Positioning the client on her side can improve blood flow and oxygen delivery to the placenta and fetus by relieving pressure on the vena cava and aorta.
B. Elevate the client's legs.
Choice B reason: Elevate the client's legs is incorrect, as this is not a priority action for a client who has late decelerations. Elevating the legs can increase venous return and cardiac output, but it can also reduce blood flow and oxygen delivery to the placenta and fetus by compressing the vena cava and aorta.
C. Administer oxygen via face mask.
Choice C reason: Administer oxygen via face mask is incorrect, as this is not the first action the nurse should take, although it is important to do later. Administering oxygen can increase oxygen saturation and delivery to the placenta and fetus, but it does not address the cause of uteroplacental insufficiency or improve blood flow.
D. Increase the infusion rate of the IV fluid.
Choice D reason: Increase the infusion rate of the IV fluid is incorrect, as this is not the first action the nurse should take, although it may be indicated later. Increasing the infusion rate of IV fluid can expand blood volume and improve placental perfusion, but it does not address the cause of uteroplacental insufficiency or improve blood flow. The nurse should obtain a provider's order before increasing the IV fluid rate.
Full Explanation
Choice A reason: Position the client on her side is correct, as this is the first action the nurse should take according to the ABCDE priority framework. Late decelerations are symmetrical decreases in the fetal heart rate that begin after the peak of the contraction and return to baseline after the contraction ends, which indicate uteroplacental insufficiency and fetal hypoxia. Positioning the client on her side can improve blood flow and oxygen delivery to the placenta and fetus by relieving pressure on the vena cava and aorta.
Choice B reason: Elevate the client's legs is incorrect, as this is not a priority action for a client who has late decelerations. Elevating the legs can increase venous return and cardiac output, but it can also reduce blood flow and oxygen delivery to the placenta and fetus by compressing the vena cava and aorta.
Choice C reason: Administer oxygen via face mask is incorrect, as this is not the first action the nurse should take, although it is important to do later. Administering oxygen can increase oxygen saturation and delivery to the placenta and fetus, but it does not address the cause of uteroplacental insufficiency or improve blood flow.
Choice D reason: Increase the infusion rate of the IV fluid is incorrect, as this is not the first action the nurse should take, although it may be indicated later. Increasing the infusion rate of IV fluid can expand blood volume and improve placental perfusion, but it does not address the cause of uteroplacental insufficiency or improve blood flow. The nurse should obtain a provider's order before increasing the IV fluid rate.