Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is planning care for a toddler who has epiglottitis.
Which of the following interventions should the nurse include?
A. Assess the child for frequent swallowing.
wrong because assessing the child for frequent swallowing may increase the risk of vomiting and aspiration. Swallowing may also be difficult and painful for the child due to the inflammation of the epiglottis.
B. Continuously monitor the child’s respiratory status.
Continuously monitor the child’s respiratory status. This is because epiglottitis is a life-threatening condition that can cause severe airway obstruction and respiratory distress in children. The nurse should monitor the child for signs of worsening breathing, such as stridor, cyanosis, restlessness, or drooling. The nurse should also be prepared to assist with intubation or tracheostomy if needed.
C. Carefully suction the child’s oropharynx to remove secretions.
is wrong because suctioning the child’s oropharynx may cause more swelling and irritation of the epiglottis, or trigger a spasm that can close off the airway. The nurse should avoid any stimulation of the throat or mouth that may worsen the condition.
D. Administer pancreatic enzymes with meals.
The correct answer is choice B. Continuously monitor the child’s respiratory status. This is because epiglottitis is a life-threatening condition that can cause severe airway obstruction and respiratory distress in children. The nurse should monitor the child for signs of worsening breathing, such as stridor, cyanosis, restlessness, or drooling. The nurse should also be prepared to assist with intubation or tracheostomy if needed. Choice A is wrong because assessing the child for frequent swallowing may increase the risk of vomiting and aspiration. Swallowing may also be difficult and painful for the child due to the inflammation of the epiglottis. Choice C is wrong because suctioning the child’s oropharynx may cause more swelling and irritation of the epiglottis, or trigger a spasm that can close off the airway. The nurse should avoid any stimulation of the throat or mouth that may worsen the condition. Choice D is wrong because administering pancreatic enzymes with meals is not relevant to epiglottitis. Pancreatic enzymes are used to treat cystic fibrosis, a genetic disorder that affects the lungs and digestive system. Epiglottitis is caused by a bacterial infection or an injury to the throat.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Comprehensive Predictor 2023 Exit Proctored Exam A. Take the full exam now
Full Explanation
The correct answer is choice B. Continuously monitor the child’s respiratory status. This is because epiglottitis is a life-threatening condition that can cause severe airway obstruction and respiratory distress in children. The nurse should monitor the child for signs of worsening breathing, such as stridor, cyanosis, restlessness, or drooling. The nurse should also be prepared to assist with intubation or tracheostomy if needed.
Choice A is wrong because assessing the child for frequent swallowing may increase the risk of vomiting and aspiration. Swallowing may also be difficult and painful for the child due to the inflammation of the epiglottis.
Choice C is wrong because suctioning the child’s oropharynx may cause more swelling and irritation of the epiglottis, or trigger a spasm that can close off the airway. The nurse should avoid any stimulation of the throat or mouth that may worsen the condition.
Choice D is wrong because administering pancreatic enzymes with meals is not relevant to epiglottitis. Pancreatic enzymes are used to treat cystic fibrosis, a genetic disorder that affects the lungs and digestive system. Epiglottitis is caused by a bacterial infection or an injury to the throat.
Similar Questions
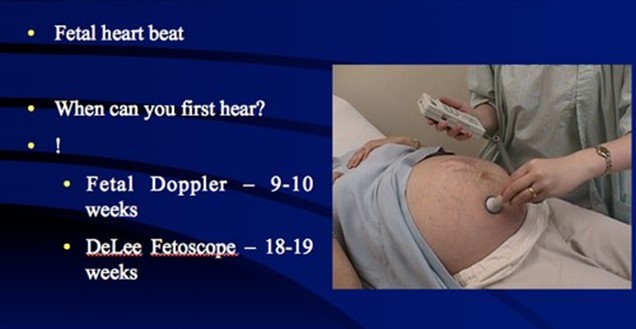
A nurse is preparing to assess fetal heart tones for a client who is at 12 weeks of gestation.
Which of the following actions should the nurse take?
A. Position the ultrasound stethoscope above the symphysis pubis to assess the fetal heart rate.
This is because at 12 weeks of gestation, the uterus is still low in the pelvis and the fetal heart tones are best audible through the fetal back, which is usually located just above the symphysis pubis. The fetal heart rate at this stage is normally between 120 and 180 beats per minute.
B. Measure the fundal height to determine the placement of the ultrasound stethoscope.
because measuring the fundal height is not necessary to determine the placement of the ultrasound stethoscope at 12 weeks of gestation. The fundal height is usually measured from 20 weeks of gestation onwards to assess fetal growth and estimate gestational age.
C. Place the client in a side-lying position prior to assessing the fetal heart rate.
wrong because placing the client in a side-lying position prior to assessing the fetal heart rate is not required at 12 weeks of gestation. This position may be helpful later in pregnancy to improve maternal blood flow and oxygen delivery to the fetus, especially if there are signs of fetal distress or hypoxia.
D. Perform Leopold maneuvers prior to auscultating the fetal heart rate.
because performing Leopold maneuvers prior to auscultating the fetal heart rate is not appropriate at 12 weeks of gestation. Leopold maneuvers are a series of four steps to palpate the abdomen and determine the fetal position, presentation, lie, and engagement. They are usually performed after 24 weeks of gestation when the fetus is large enough to be felt through the abdominal wall.
Full Explanation
A nurse is caring for a child who is postoperative following a tonsillectomy.
Which of the following findings indicates that the child may be experiencing hemorrhage?
A. Elevated pain level.
because elevated pain level is not a specific sign of hemorrhage. Pain is expected after a tonsillectomy and can be managed with medication and fluids.
B. Increased drowsiness.
because increased drowsiness is not a specific sign of hemorrhage. Drowsiness can be caused by anesthesia, medication, or dehydration.
C. Frequent swallowing.
This indicates that the child may be experiencing hemorrhage because they are trying to clear the blood from their throat. Frequent swallowing is one of the initial signs of bleeding immediately after tonsillectomy.
D. Diminished breath sounds.
because diminished breath sounds are not a specific sign of hemorrhage. Diminished breath sounds can be caused by respiratory infection, asthma, or bronchospasm. Normal ranges for hemoglobin and hematocrit are 11.5 to 15.5 g/dL and 34 to 45% for children, respectively. Normal ranges for platelet count are 150,000 to 450,000/mm3 for both children and adults. Normal ranges for plasma clotting variables depend on the specific test and method used.
Full Explanation
The correct answer is choice C, frequent swallowing.
This indicates that the child may be experiencing hemorrhage because they are trying to clear the blood from their throat. Frequent swallowing is one of the initial signs of bleeding immediately after tonsillectomy.
Choice A is wrong because elevated pain level is not a specific sign of hemorrhage.
Pain is expected after a tonsillectomy and can be managed with medication and fluids.
Choice B is wrong because increased drowsiness is not a specific sign of hemorrhage.
Drowsiness can be caused by anesthesia, medication, or dehydration.
Choice D is wrong because diminished breath sounds are not a specific sign of hemorrhage.
Diminished breath sounds can be caused by respiratory infection, asthma, or bronchospasm.
Normal ranges for hemoglobin and hematocrit are 11.5 to 15.5 g/dL and 34 to 45% for children, respectively.
Normal ranges for platelet count are 150,000 to 450,000/mm3 for both children and adults.
Normal ranges for plasma clotting variables depend on the specific test and method used.
A nurse is assessing a client who is taking haloperidol and is experiencing pseudoparkinsonism.
Which of the following findings should the nurse document as a manifestation of pseudoparkinsonism?
A. Nonreactive pupils.
Nonreactive pupils is wrong because this is not a typical feature of pseudoparkinsonism or Parkinson’s disease. Nonreactive pupils can be caused by other conditions, such as brain injury, drugs, or eye diseases.
B. Serpentine limb movement.
.Serpentine limb movement is wrong because this is a characteristic of tardive dyskinesia, another drug-induced movement disorder that can result from long-term use of dopamine receptor blocking agents. Tardive dyskinesia causes involuntary movements of the face, tongue, and limbs that are often writhing or twisting
C. Smacking lips.
Smacking lips is wrong because this is also a sign of tardive dyskinesia, not pseudoparkinsonism. Smacking lips is one of the orofacial movements that can occur in tardive dyskinesia due to abnormal muscle contractions.
D. Shuffling gait.
This is because shuffling gait is a common manifestation of pseudoparkinsonism, which is a condition that mimics the symptoms of Parkinson’s disease due to the use of certain medications that block dopamine receptors, such as haloperidol. Pseudoparkinsonism can cause slowed movements, muscle stiffness, tremor, and postural instability.
Full Explanation
The correct answer is choice D. Shuffling gait. This is because shuffling gait is a common manifestation of pseudoparkinsonism, which is a condition that mimics the symptoms of Parkinson’s disease due to the use of certain medications that block dopamine receptors, such as haloperidol. Pseudoparkinsonism can cause slowed movements, muscle stiffness, tremor, and postural instability.
Choice A. Nonreactive pupils is wrong because this is not a typical feature of pseudoparkinsonism or Parkinson’s disease.
Nonreactive pupils can be caused by other conditions, such as brain injury, drugs, or eye diseases.
Choice B. Serpentine limb movement is wrong because this is a characteristic of tardive dyskinesia, another drug-induced movement disorder that can result from long-term use of dopamine receptor blocking agents. Tardive dyskinesia causes involuntary movements of the face, tongue, and limbs that are often writhing or twisting.
Choice C. Smacking lips is wrong because this is also a sign of tardive dyskinesia, not pseudoparkinsonism. Smacking lips is one of the orofacial movements that can occur in tardive dyskinesia due to abnormal muscle contractions.