Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is providing dietary teaching for a client who has chronic obstructive pulmonary disease. Which of the following instructions should the nurse include?
A. "Use a bronchodilator 1 hour before eating."
A. Administration of a prescribed bronchodilator is typically recommended approximately 30 minutes prior to meals rather than 1 hour. This pharmacological timing helps reduce dyspnea and facilitates easier deglutition and mastication by improving airflow. Using it too early may result in the peak therapeutic effect tapering off before the client finishes the meal.
B. "Eat 3 large meals each day."
B. Consuming 3 large meals each day is contraindicated for clients with chronic obstructive pulmonary disease because a distended stomach can exert upward pressure on the diaphragm. This abdominal crowding significantly increases the work of breathing and leads to early satiety or respiratory distress. Clients are instead encouraged to eat 5 to 6 small, frequent, nutrient-dense meals.
C. "Limit water intake with meals."
C. The nurse should instruct the client to limit water or fluid intake during the actual mealtime to prevent premature gastric distention. Early fullness from fluids reduces the client’s ability to consume essential solid nutrients and calories required to support the increased metabolic demands of labored breathing. Fluids should be consumed between meals to maintain adequate hydration and thin secretions.
D. "Reduce protein intake."
D. Reducing protein intake is inappropriate because these clients require high-protein and high-calorie diets to prevent muscle wasting and support the respiratory muscles. The metabolic cost of breathing in chronic obstructive pulmonary disease is significantly elevated, often leading to a state of malnutrition or cachexia. Protein is vital for tissue repair and maintaining the functional integrity of the diaphragm.
E. None
None
F. None
None
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Proctored Exam 1. Take the full exam now
Full Explanation
A. Administration of a prescribed bronchodilator is typically recommended approximately 30 minutes prior to meals rather than 1 hour. This pharmacological timing helps reduce dyspnea and facilitates easier deglutition and mastication by improving airflow. Using it too early may result in the peak therapeutic effect tapering off before the client finishes the meal.
B. Consuming 3 large meals each day is contraindicated for clients with chronic obstructive pulmonary disease because a distended stomach can exert upward pressure on the diaphragm. This abdominal crowding significantly increases the work of breathing and leads to early satiety or respiratory distress. Clients are instead encouraged to eat 5 to 6 small, frequent, nutrient-dense meals.
C. The nurse should instruct the client to limit water or fluid intake during the actual mealtime to prevent premature gastric distention. Early fullness from fluids reduces the client’s ability to consume essential solid nutrients and calories required to support the increased metabolic demands of labored breathing. Fluids should be consumed between meals to maintain adequate hydration and thin secretions.
D. Reducing protein intake is inappropriate because these clients require high-protein and high-calorie diets to prevent muscle wasting and support the respiratory muscles. The metabolic cost of breathing in chronic obstructive pulmonary disease is significantly elevated, often leading to a state of malnutrition or cachexia. Protein is vital for tissue repair and maintaining the functional integrity of the diaphragm.
Similar Questions
A nurse is caring for a client who has a chest tube connected to a closed drainage system and needs to be transported to the x-ray department. Which of the following actions should the nurse take?
A. Disconnect the chest tube from the drainage system during transport.
Disconnecting the chest tube from the drainage system during transport is dangerous and can cause pneumothorax, infection, or bleeding. The chest tube should remain connected to the drainage system at all times unless ordered by the provider.
B. Empty the collection chamber prior to transport.
Emptying the collection chamber prior to transport is unnecessary and can interfere with accurate measurement of drainage. The collection chamber should be emptied only when it is full or at the end of each shift.
C. Clamp the chest tube prior to transferring the client to a wheelchair.
Clamping the chest tube prior to transferring the client to a wheelchair is contraindicated and can cause tension pneumothorax, as it prevents air from escaping the pleural space. The chest tube should only be clamped for a brief period when changing the drainage system or checking for air leaks, and only with a provider's order.
D. Keep the drainage system below the level of the client's chest at all times.
Keeping the drainage system below the level of the client's chest prevents backflow of fluid or air into the pleural space and maintains negative pressure in the system.
Full Explanation
Keeping the drainage system below the level of the client's chest prevents backflow of fluid or air into the pleural space and maintains negative pressure in the system.
a) Disconnecting the chest tube from the drainage system during transport is dangerous and can cause pneumothorax, infection, or bleeding. The chest tube should remain connected to the drainage system at all times unless ordered by the provider.
b) Emptying the collection chamber prior to transport is unnecessary and can interfere with accurate measurement of drainage. The collection chamber should be emptied only when it is full or at the end of each shift.
c) Clamping the chest tube prior to transferring the client to a wheelchair is contraindicated and can cause tension pneumothorax, as it prevents air from escaping the pleural space. The chest tube should only be clamped for a brief period when changing the drainage system or checking for air leaks, and only with a provider's order.
A nurse on a medical-surgical unit is performing an admission assessment of a client who has COPD with emphysema. The client reports that he has a frequent productive cough and is short of breath. The nurse should anticipate which of the following assessment findings for this client?
A. Oxygen saturation level 96%
Oxygen saturation level 96% is within the normal range of 95% to 100% and does not indicate hypoxemia or impaired gas exchange. Clients who have COPD with emphysema typically have lower oxygen saturation levels, ranging from 88% to 92%.
B. Respiratory alkalosis
Respiratory alkalosis is a condition in which the blood pH is elevated due to decreased carbon dioxide levels. It is caused by hyperventilation, which can occur in response to hypoxia, anxiety, or pain. Clients who have COPD with emphysema usually have respiratory acidosis, which is a condition in which the blood pH is lowered due to increased carbon dioxide levels. It is caused by hypoventilation, which results from impaired lung function and airway obstruction.
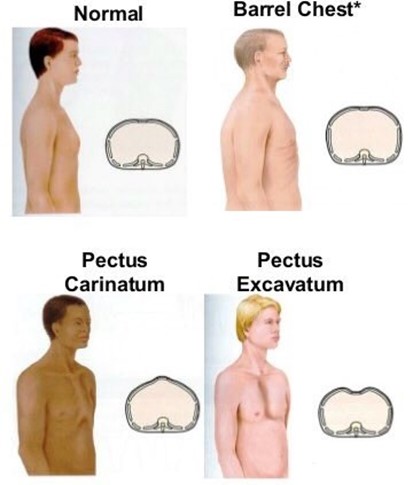
C. Increased anteroposterior diameter of the chest
Increased anteroposterior diameter of the chest, also known as barrel chest, is a common finding in clients who have COPD with emphysema. It is caused by chronic air trapping and hyperinflation of the lungs, which results in fattening of the diaphragm and widening of the rib cage.
D. Petechiae on chest
Petechiae on chest are small red or purple spots on the skin caused by bleeding from capillaries. They are not a typical finding in clients who have COPD with emphysema, unless they have severe coughing episodes or coagulation disorders. They can indicate infection, inflammation, trauma, or vascular disease.
Full Explanation
Increased anteroposterior diameter of the chest, also known as barrel chest, is a common finding in clients who have COPD with emphysema. It is caused by chronic air trapping and hyperinflation of the lungs, which results in fattening of the diaphragm and widening of the rib cage.
a) Oxygen saturation level 96% is within the normal range of 95% to 100% and does not indicate hypoxemia or impaired gas exchange. Clients who have COPD with emphysema typically have lower oxygen saturation levels, ranging from 88% to 92%.
b) Respiratory alkalosis is a condition in which the blood pH is elevated due to decreased carbon dioxide levels. It is caused by hyperventilation, which can occur in response to hypoxia, anxiety, or pain. Clients who have COPD with emphysema usually have respiratory acidosis, which is a condition in which the blood pH is lowered due to increased carbon dioxide levels. It is caused by hypoventilation, which results from impaired lung function and airway obstruction.
d) Petechiae on chest are small red or purple spots on the skin caused by bleeding from capillaries. They are not a typical finding in clients who have COPD with emphysema, unless they have severe coughing episodes or coagulation disorders. They can indicate infection, inflammation, trauma, or vascular disease.
A nurse is caring for a client who has asthma and is taking fluticasone. The nurse should monitor the client
for which of the following adverse effects?
A. Polyuria
Polyuria, or excessive urination, is not an adverse effect of fluticasone. It can be caused by diabetes mellitus, diabetes insipidus, diuretics, or kidney disease.
B. Hypoglycemia
Hypoglycemia, or low blood glucose level, is not an adverse effect of fluticasone. It can be caused by insulin overdose, oral hypoglycemic agents, alcohol intake, or prolonged fasting.
C. Hypertension
Hypertension, or high blood pressure, is not an adverse effect of fluticasone. It can be caused by stress, obesity, smoking, salt intake, or kidney disease.
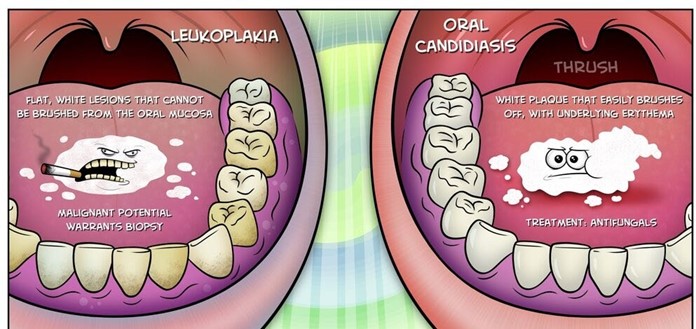
D. Oral candidiasis
Oral candidiasis, also known as thrush, is a fungal infection of the mouth caused by Candida albicans. It is a common adverse effect of inhaled corticosteroids, such as fluticasone, which can suppress the normal flora of the oral cavity and create a favorable environment for fungal growth. It manifests as white patches or plaques on the tongue, palate, or cheeks that can be scraped off.
Full Explanation
Oral candidiasis, also known as thrush, is a fungal infection of the mouth caused by Candida albicans. It is a common adverse effect of inhaled corticosteroids, such as fluticasone, which can suppress the normal flora of the oral cavity and create a favorable environment for fungal growth. It manifests as white patches or plaques on the tongue, palate, or cheeks that can be scraped off.
a) Polyuria, or excessive urination, is not an adverse effect of fluticasone. It can be caused by diabetes mellitus, diabetes insipidus, diuretics, or kidney disease.
b) Hypoglycemia, or low blood glucose level, is not an adverse effect of fluticasone. It can be caused by
insulin overdose, oral hypoglycemic agents, alcohol intake, or prolonged fasting.
c) Hypertension, or high blood pressure, is not an adverse effect of fluticasone. It can be caused by stress, obesity, smoking, salt intake, or kidney disease.