Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is providing education to a community group about burn prevention. Which of the following is an example of a first-degree burn?
A. Excessive scarring
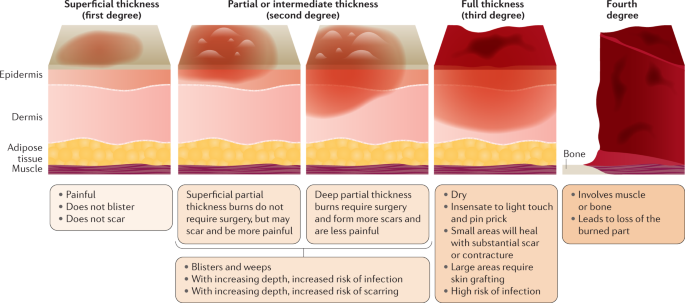
Excessive scarring:Excessive scarring is not an example of a first-degree burn. It typically occurs in more severe burns that affect deeper layers of the skin, such as second-degree or third-degree burns. Second-degree burns extend into the dermis, while third-degree burns damage all layers of the skin and can lead to significant scarring. First-degree burns, on the other hand, only affect the outer layer of the skin (epidermis) and usually do not result in excessive scarring.
B. Blistering from flames
Blistering from flames:Blistering from flames is more characteristic of a second-degree burn rather than a first-degree burn. Second-degree burns involve damage to both the epidermis and part of the dermis, which can result in blister formation. These burns are often caused by direct contact with flames, hot liquids, or steam.
C. Blackened dead skin
Blackened dead skin: Blackened dead skin is indicative of a third-degree burn, which is the most severe type of burn. Third-degree burns damage all layers of the skin, including the epidermis, dermis, and sometimes underlying tissues. The skin may appear charred or blackened, and these burns often require medical intervention, such as skin grafting, due to the extent of tissue damage.
D. A sunburn
A sunburn:A sunburn is an example of a first-degree burn. It occurs due to overexposure to ultraviolet (UV) radiation from the sun, leading to redness, pain, and mild swelling of the skin. First-degree burns affect only the outer layer of the skin (epidermis) and typically heal within a few days without significant scarring or blistering. Applying soothing lotions, staying hydrated, and avoiding further sun exposure can help manage sunburns.
This question is an excerpt from Nurse Dive's nursing test bank - Ati Lpn Med Surg Cohort 6 Proctored Exam. Take the full exam now
Full Explanation
A. Excessive scarring:
Excessive scarring is not an example of a first-degree burn. It typically occurs in more severe burns that affect deeper layers of the skin, such as second-degree or third-degree burns. Second-degree burns extend into the dermis, while third-degree burns damage all layers of the skin and can lead to significant scarring. First-degree burns, on the other hand, only affect the outer layer of the skin (epidermis) and usually do not result in excessive scarring.
B. Blistering from flames:
Blistering from flames is more characteristic of a second-degree burn rather than a first-degree burn. Second-degree burns involve damage to both the epidermis and part of the dermis, which can result in blister formation. These burns are often caused by direct contact with flames, hot liquids, or steam.
C. Blackened dead skin:
Blackened dead skin is indicative of a third-degree burn, which is the most severe type of burn. Third-degree burns damage all layers of the skin, including the epidermis, dermis, and sometimes underlying tissues. The skin may appear charred or blackened, and these burns often require medical intervention, such as skin grafting, due to the extent of tissue damage.
D. A sunburn:
A sunburn is an example of a first-degree burn. It occurs due to overexposure to ultraviolet (UV) radiation from the sun, leading to redness, pain, and mild swelling of the skin. First-degree burns affect only the outer layer of the skin (epidermis) and typically heal within a few days without significant scarring or blistering. Applying soothing lotions, staying hydrated, and avoiding further sun exposure can help manage sunburns.
Similar Questions
The nurse is caring for a client with a chronic wound. Which of the following are wound treatments that may assist with the healing process?
A. Measure the depth and width of the wound.
Measure the depth and width of the wound. Regular assessment and documentation of the wound’s size can help track the progress of healing and effectiveness of the treatment plan.
B. Educate the client about the need for antibiotics.
Educate the client about the need for antibiotics. If an infection is present, antibiotics may be necessary. It’s important for the client to understand the purpose and proper use of these medications.
C. Consult a nutritionist for a diet plan.
Consult a nutritionist for a diet plan. Good nutrition is essential for wound healing. Certain nutrients, like protein, vitamin C, and zinc, can promote wound healing.
D. Remove any non-viable tissue.
Remove any non-viable tissue. Debridement, or the removal of dead (non-viable) tissue, can help promote the healing of the wound by reducing the risk of infection and allowing healthy tissue to grow.
Full Explanation
-
A. Measure the depth and width of the wound. Regular assessment and documentation of the wound’s size can help track the progress of healing and effectiveness of the treatment plan.
B. Educate the client about the need for antibiotics. If an infection is present, antibiotics may be necessary. It’s important for the client to understand the purpose and proper use of these medications.
C. Consult a nutritionist for a diet plan. Good nutrition is essential for wound healing. Certain nutrients, like protein, vitamin C, and zinc, can promote wound healing.
D. Remove any non-viable tissue. Debridement, or the removal of dead (non-viable) tissue, can help promote the healing of the wound by reducing the risk of infection and allowing healthy tissue to grow.
Melanocytes give rise to the pigment melanin, which is responsible for skin color. Where can the melanocytes be found?
A. Loose connective tissue
Loose connective tissue:Melanocytes are not typically found in loose connective tissue. Their primary location is within the epidermis, specifically in the basal layer, where they interact with keratinocytes to produce melanin and contribute to skin color. Loose connective tissue contains collagen and elastin fibers, as well as fibroblasts, but it does not house melanocytes.
B. Epidermis
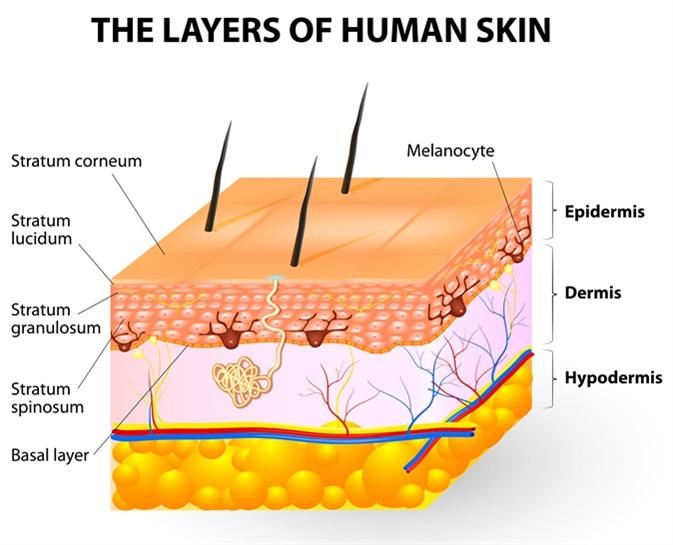
Epidermis: This is the correct answer. Melanocytes are primarily located in the basal layer of the epidermis, which is the deepest layer of the epidermis. These cells produce melanin, a pigment that helps protect the skin from UV radiation and determines skin color. Melanocytes are interspersed among keratinocytes in the epidermis and transfer melanin to keratinocytes to provide skin pigmentation.
C. Dermis
Dermis:The dermis is the layer of skin beneath the epidermis and consists of connective tissue, blood vessels, nerves, hair follicles, and sweat glands. While the dermis plays a crucial role in supporting and nourishing the epidermis, melanocytes are not primarily located in the dermis. They are confined to the basal layer of the epidermis.
D. Superficial fascia
Superficial fascia:The superficial fascia, also known as the subcutaneous tissue or hypodermis, lies beneath the dermis and consists of adipose (fat) tissue and connective tissue. It provides insulation, energy storage, and cushioning for underlying structures. However, melanocytes are not typically found in the superficial fascia. They are restricted to the epidermis, specifically the basal layer, where they carry out their function of melanin production.
Full Explanation
A. Loose connective tissue:
Melanocytes are not typically found in loose connective tissue. Their primary location is within the epidermis, specifically in the basal layer, where they interact with keratinocytes to produce melanin and contribute to skin color. Loose connective tissue contains collagen and elastin fibers, as well as fibroblasts, but it does not house melanocytes.
B. Epidermis:
This is the correct answer. Melanocytes are primarily located in the basal layer of the epidermis, which is the deepest layer of the epidermis. These cells produce melanin, a pigment that helps protect the skin from UV radiation and determines skin color. Melanocytes are interspersed among keratinocytes in the epidermis and transfer melanin to keratinocytes to provide skin pigmentation.
C. Dermis:
The dermis is the layer of skin beneath the epidermis and consists of connective tissue, blood vessels, nerves, hair follicles, and sweat glands. While the dermis plays a crucial role in supporting and nourishing the epidermis, melanocytes are not primarily located in the dermis. They are confined to the basal layer of the epidermis.
D. Superficial fascia:
The superficial fascia, also known as the subcutaneous tissue or hypodermis, lies beneath the dermis and consists of adipose (fat) tissue and connective tissue. It provides insulation, energy storage, and cushioning for underlying structures. However, melanocytes are not typically found in the superficial fascia. They are restricted to the epidermis, specifically the basal layer, where they carry out their function of melanin production.
A nurse is caring for a client during fluid resuscitation for burns. Which of the following are used to evaluate the success of fluid resuscitation? (Select all that apply.)
A. Blood pressure
Blood pressure:Monitoring blood pressure is a crucial aspect of evaluating fluid resuscitation in burn patients. Adequate fluid resuscitation should help maintain stable blood pressure levels within an acceptable range. Hypotension (low blood pressure) can indicate inadequate fluid resuscitation, leading to poor tissue perfusion and organ function. On the other hand, hypertension (high blood pressure) may suggest fluid overload, which can lead to complications such as pulmonary edema. Therefore, regular monitoring of blood pressure helps assess the effectiveness of fluid resuscitation and guides adjustments in fluid administration rates.
B. Bowel sounds
Bowel sounds:While bowel sounds are important indicators of gastrointestinal motility and function, they are not directly used to evaluate the success of fluid resuscitation in burn patients. Bowel sounds may be assessed for other reasons, such as postoperative recovery or gastrointestinal conditions, but they do not provide specific information about fluid resuscitation status or tissue perfusion.
C. Level of consciousness
Level of consciousness:Assessing the client's level of consciousness is crucial during fluid resuscitation for burns. Changes in consciousness, such as confusion, lethargy, or altered mental status, can indicate inadequate tissue perfusion and oxygenation. A clear and responsive level of consciousness suggests adequate fluid resuscitation and perfusion to vital organs, while alterations in consciousness may prompt further evaluation and adjustment of fluid resuscitation strategies.
D. Urine output
Urine output:Monitoring urine output is a key parameter in evaluating fluid resuscitation in burn patients. Adequate urine output (0.5 to 1 mL/kg/hr in adults) indicates sufficient renal perfusion and function, suggesting effective fluid resuscitation. Decreased urine output or oliguria may indicate inadequate fluid resuscitation, renal impairment, or hypovolemia, requiring reassessment and potential adjustments in fluid administration rates or type of fluids used.
E. Platelet count
Platelet count is an important component of the complete blood count (CBC) and is used to assess clotting function and risk of bleeding. However, platelet count is not specifically used to evaluate the success of fluid resuscitation in burn patients. While clotting parameters may be monitored in burn patients, including platelet count, they are not direct indicators of fluid resuscitation status or tissue perfusion. Other laboratory parameters, such as hemoglobin, hematocrit, electrolyte levels, and arterial blood gases, may be monitored to assess the effectiveness of fluid resuscitation.
Full Explanation
A. Blood pressure:
Monitoring blood pressure is a crucial aspect of evaluating fluid resuscitation in burn patients. Adequate fluid resuscitation should help maintain stable blood pressure levels within an acceptable range. Hypotension (low blood pressure) can indicate inadequate fluid resuscitation, leading to poor tissue perfusion and organ function. On the other hand, hypertension (high blood pressure) may suggest fluid overload, which can lead to complications such as pulmonary edema. Therefore, regular monitoring of blood pressure helps assess the effectiveness of fluid resuscitation and guides adjustments in fluid administration rates.
B. Bowel sounds:
While bowel sounds are important indicators of gastrointestinal motility and function, they are not directly used to evaluate the success of fluid resuscitation in burn patients. Bowel sounds may be assessed for other reasons, such as postoperative recovery or gastrointestinal conditions, but they do not provide specific information about fluid resuscitation status or tissue perfusion.
C. Level of consciousness:
Assessing the client's level of consciousness is crucial during fluid resuscitation for burns. Changes in consciousness, such as confusion, lethargy, or altered mental status, can indicate inadequate tissue perfusion and oxygenation. A clear and responsive level of consciousness suggests adequate fluid resuscitation and perfusion to vital organs, while alterations in consciousness may prompt further evaluation and adjustment of fluid resuscitation strategies.
D. Urine output:
Monitoring urine output is a key parameter in evaluating fluid resuscitation in burn patients. Adequate urine output (0.5 to 1 mL/kg/hr in adults) indicates sufficient renal perfusion and function, suggesting effective fluid resuscitation. Decreased urine output or oliguria may indicate inadequate fluid resuscitation, renal impairment, or hypovolemia, requiring reassessment and potential adjustments in fluid administration rates or type of fluids used.
E. Platelet count:
Platelet count is an important component of the complete blood count (CBC) and is used to assess clotting function and risk of bleeding. However, platelet count is not specifically used to evaluate the success of fluid resuscitation in burn patients. While clotting parameters may be monitored in burn patients, including platelet count, they are not direct indicators of fluid resuscitation status or tissue perfusion. Other laboratory parameters, such as hemoglobin, hematocrit, electrolyte levels, and arterial blood gases, may be monitored to assess the effectiveness of fluid resuscitation.