Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A. Feedings should be accompanied by nonnutritive sucking.
Feedings should not be accompanied by nonnutritive sucking. Nonnutritive sucking is the act of sucking on a pacifier, finger, or other object without getting any nutrition. Nonnutritive sucking can interfere with the establishment of breastfeeding, cause nipple confusion, and reduce milk supply.
B. Feedings should be on demand.
Feedings should be on demand. On demand feeding means feeding the newborn whenever they show signs of hunger, such as rooting, sucking, or crying. On demand feeding helps the newborn regulate their appetite, meet their nutritional needs, and bond with their caregiver.
C. Feedings should begin within 1 hr after birth.
Feedings should not begin within 1 hr after birth. This instruction is applicable for breastfeeding, not bottle feeding. Breastfeeding should begin within 1 hr after birth to initiate milk production, stimulate uterine contractions, and transfer colostrum to the newborn. Bottle feeding can be delayed until the newborn is stable and alert.
D. Feedings may occur in clusters.
Feedings may not occur in clusters. Cluster feeding means feeding the newborn more frequently and for longer periods of time during certain times of the day or night. Cluster feeding is common in breastfed newborns, especially during growth spurts or developmental leaps. Bottle fed newborns may not exhibit cluster feeding, as they tend to have more consistent and predictable feeding patterns.
This question is an excerpt from Nurse Dive's nursing test bank - RN Nutrition 2019 Nexy Updated 2023 Proctored Exam. Take the full exam now
Full Explanation
Choice A reason: Feedings should not be accompanied by nonnutritive sucking. Nonnutritive sucking is the act of sucking on a pacifier, finger, or other object without getting any nutrition. Nonnutritive sucking can interfere with the establishment of breastfeeding, cause nipple confusion, and reduce milk supply.
Choice B reason: Feedings should be on demand. On demand feeding means feeding the newborn whenever they show signs of hunger, such as rooting, sucking, or crying. On demand feeding helps the newborn regulate their appetite, meet their nutritional needs, and bond with their caregiver.
Choice C reason: Feedings should not begin within 1 hr after birth. This instruction is applicable for breastfeeding, not bottle feeding. Breastfeeding should begin within 1 hr after birth to initiate milk production, stimulate uterine contractions, and transfer colostrum to the newborn. Bottle feeding can be delayed until the newborn is stable and alert.
Choice D reason: Feedings may not occur in clusters. Cluster feeding means feeding the newborn more frequently and for longer periods of time during certain times of the day or night. Cluster feeding is common in breastfed newborns, especially during growth spurts or developmental leaps. Bottle fed newborns may not exhibit cluster feeding, as they tend to have more consistent and predictable feeding patterns.
Similar Questions
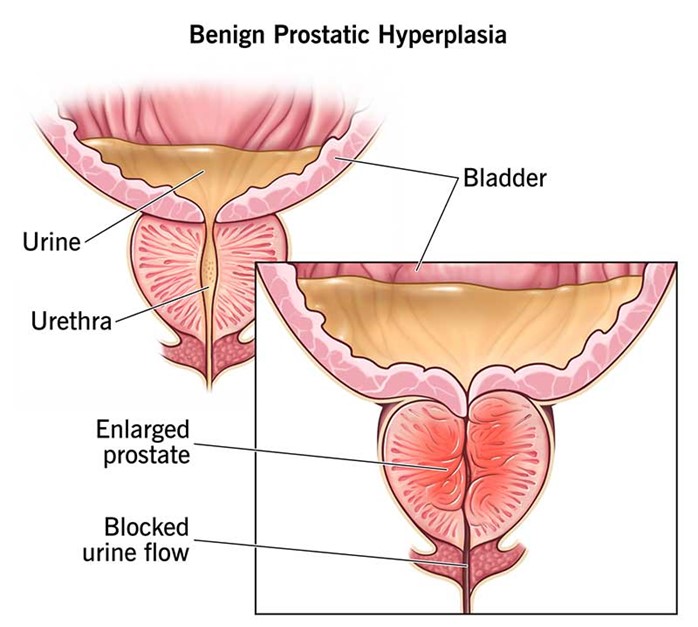
A nurse is caring for a client who has benign prostatic hyperplasia. Which of the following findings indicates that the client's treatment has been effective?
A. The client has a creatinine level of 1.0 mg/dL.
The client's creatinine level of 1.0 mg/dL is within the normal range (0.6-1.2), but it does not indicate the effectiveness of the treatment for benign prostatic hyperplasia. Creatinine is a waste product of muscle metabolism that is filtered by the kidneys. High creatinine levels can indicate kidney damage or impaired renal function.
B. The client has a urine output of 35 mL/hr.
The client's urine output of 35 mL/hr is below the normal range (40-60), and it indicates the need for further assessment. Low urine output can indicate dehydration, urinary retention, or kidney failure.
C. The client passes soft, brown stool.
The client's stool consistency and color are not related to the treatment for benign prostatic hyperplasia. Soft, brown stool is normal and does not indicate any problem with the digestive system.
D. The client does not have to strain to begin urination.
The client's ability to urinate without straining indicates that the treatment for benign prostatic hyperplasia has been effective. Benign prostatic hyperplasia is a condition in which the prostate gland enlarges and compresses the urethra, causing difficulty in urination. Treatment options include medication, surgery, or minimally invasive procedures to reduce the size of the prostate and relieve urinary obstruction.
Full Explanation
Choice A reason: The client's creatinine level of 1.0 mg/dL is within the normal range (0.6-1.2), but it does not indicate the effectiveness of the treatment for benign prostatic hyperplasia. Creatinine is a waste product of muscle metabolism that is filtered by the kidneys. High creatinine levels can indicate kidney damage or impaired renal function.
Choice B reason: The client's urine output of 35 mL/hr is below the normal range (40-60), and it indicates the need for further assessment. Low urine output can indicate dehydration, urinary retention, or kidney failure.
Choice C reason: The client's stool consistency and color are not related to the treatment for benign prostatic hyperplasia. Soft, brown stool is normal and does not indicate any problem with the digestive system.
Choice D reason: The client's ability to urinate without straining indicates that the treatment for benign prostatic hyperplasia has been effective. Benign prostatic hyperplasia is a condition in which the prostate gland enlarges and compresses the urethra, causing difficulty in urination. Treatment options include medication, surgery, or minimally invasive procedures to reduce the size of the prostate and relieve urinary obstruction.
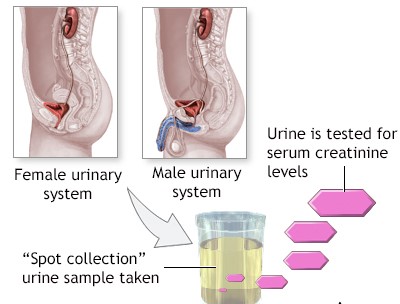
A nurse is reviewing the laboratory reports of a client who is undergoing nutritional screening due to a risk for chronic kidney disease. The nurse should identify that which of the following results indicates the need for further assessment?
A. Serum creatinine 3.5 mg/dL
Serum creatinine 3.5 mg/dL is high and indicates the need for further assessment. Creatinine is a waste product of muscle metabolism that is filtered by the kidneys. High creatinine levels can indicate kidney damage or impaired renal function.
B. Hematocrit 45%
Hematocrit 45% is within the normal range (37-47% for women, 40-50% for men), and it does not indicate the need for further assessment. Hematocrit is the percentage of red blood cells in the blood. Low hematocrit levels can indicate anemia, bleeding, or hemolysis.
C. Blood urea nitrogen 18 mg/dL
Blood urea nitrogen 18 mg/dL is within the normal range (7-20), and it does not indicate the need for further assessment. Blood urea nitrogen is a waste product of protein metabolism that is filtered by the kidneys. High blood urea nitrogen levels can indicate dehydration, kidney damage, or high protein intake.
D. Sodium 140 mEq/L
Sodium 140 mEq/L is within the normal range (135-145), and it does not indicate the need for further assessment. Sodium is an electrolyte that helps maintain fluid balance, blood pressure, and nerve impulses. Low or high sodium levels can cause confusion, seizures, or coma.
Full Explanation
Choice A reason: Serum creatinine 3.5 mg/dL is high and indicates the need for further assessment. Creatinine is a waste product of muscle metabolism that is filtered by the kidneys. High creatinine levels can indicate kidney damage or impaired renal function.
Choice B reason: Hematocrit 45% is within the normal range (37-47% for women, 40-50% for men), and it does not indicate the need for further assessment. Hematocrit is the percentage of red blood cells in the blood. Low hematocrit levels can indicate anemia, bleeding, or hemolysis.
Choice C reason: Blood urea nitrogen 18 mg/dL is within the normal range (7-20), and it does not indicate the need for further assessment. Blood urea nitrogen is a waste product of protein metabolism that is filtered by the kidneys. High blood urea nitrogen levels can indicate dehydration, kidney damage, or high protein intake.
Choice D reason: Sodium 140 mEq/L is within the normal range (135-145), and it does not indicate the need for further assessment. Sodium is an electrolyte that helps maintain fluid balance, blood pressure, and nerve impulses. Low or high sodium levels can cause confusion, seizures, or coma.
A nurse is administering continuous enteral feedings for a client through a percutaneous esophageal gastrostomy (PEG) tube. Which of the following actions should the nurse take?
A. Check gastric residuals every 8 hr.
Checking gastric residuals every 8 hr is not frequent enough, as it can miss signs of delayed gastric emptying, which can cause aspiration, nausea, vomiting, or abdominal distension. Gastric residuals should be checked every 4 hr.
B. Return gastric contents if residual is less than 250 mL.
Returning gastric contents if residual is less than 250 mL is not advisable, as it can increase the risk of infection, contamination, or electrolyte imbalance. Gastric contents should be discarded if residual is more than 100 mL.
C. Measure the pH of gastric residual every 24 hr.
Measuring the pH of gastric residual every 24 hr is not necessary, as it does not reflect the effectiveness or tolerance of the feeding. The pH of gastric residual should be checked before each feeding or every 6 to 8 hr to confirm tube placement and prevent misconnection.
D. Flush the tube with 15 mL of water every 4 hr.
Flushing the tube with 15 mL of water every 4 hr is a correct action, as it can prevent clogging, maintain patency, and clear the tube of formula residue. Water should also be used to flush the tube before and after each medication administration.
Full Explanation
Choice A reason: Checking gastric residuals every 8 hr is not frequent enough, as it can miss signs of delayed gastric emptying, which can cause aspiration, nausea, vomiting, or abdominal distension. Gastric residuals should be checked every 4 hr.
Choice B reason: Returning gastric contents if residual is less than 250 mL is not advisable, as it can increase the risk of infection, contamination, or electrolyte imbalance. Gastric contents should be discarded if residual is more than 100 mL.
Choice C reason: Measuring the pH of gastric residual every 24 hr is not necessary, as it does not reflect the effectiveness or tolerance of the feeding. The pH of gastric residual should be checked before each feeding or every 6 to 8 hr to confirm tube placement and prevent misconnection.
Choice D reason: Flushing the tube with 15 mL of water every 4 hr is a correct action, as it can prevent clogging, maintain patency, and clear the tube of formula residue. Water should also be used to flush the tube before and after each medication administration.