Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is reinforcing teaching with a client who has Crohn’s Disease and is experiencing frequent cramping and diarrhea. Which of the following statements should the nurse include in the teaching?
A. “Increase your caloric intake by eating foods high in protein.”
“Increase your caloric intake by eating foods high in protein.”This is the appropriate choice. Increasing caloric intake with high-protein foods can help meet nutritional needs for individuals with Crohn's Disease, especially if malabsorption is a concern.
B. “Include fresh fruits and vegetables at each meal.”
“Include fresh fruits and vegetables at each meal.”While fresh fruits and vegetables are generally healthy, they may exacerbate symptoms in some individuals with Crohn's Disease, especially during flare-ups. It may be advisable to choose cooked or processed fruits and vegetables to minimize irritation.
C. “Maintain your weight by eating high fat foods.”
“Maintain your weight by eating high-fat foods.” This statement is not advisable. High-fat foods can contribute to symptoms such as cramping and diarrhea in individuals with Crohn's Disease. A well-balanced diet with an appropriate mix of nutrients is generally recommended.
D. “Drink whole milk to ensure adequate calcium intake.”
“Drink whole milk to ensure adequate calcium intake.”This statement is not advisable without considering individual tolerance. Whole milk is high in fat and may be difficult to digest for some individuals with Crohn's Disease. Additionally, if lactose intolerance is present, it may worsen symptoms. Alternative sources of calcium may need to be considered.
This question is an excerpt from Nurse Dive's nursing test bank - Ati Custom Pn Basic Care And Comfort Assessment Proctored Exam. Take the full exam now
Full Explanation
A. “Increase your caloric intake by eating foods high in protein.”
This is the appropriate choice. Increasing caloric intake with high-protein foods can help meet nutritional needs for individuals with Crohn's Disease, especially if malabsorption is a concern.
B. “Include fresh fruits and vegetables at each meal.”
While fresh fruits and vegetables are generally healthy, they may exacerbate symptoms in some individuals with Crohn's Disease, especially during flare-ups. It may be advisable to choose cooked or processed fruits and vegetables to minimize irritation.
C. “Maintain your weight by eating high-fat foods.”
This statement is not advisable. High-fat foods can contribute to symptoms such as cramping and diarrhea in individuals with Crohn's Disease. A well-balanced diet with an appropriate mix of nutrients is generally recommended.
D. “Drink whole milk to ensure adequate calcium intake.”
This statement is not advisable without considering individual tolerance. Whole milk is high in fat and may be difficult to digest for some individuals with Crohn's Disease. Additionally, if lactose intolerance is present, it may worsen symptoms. Alternative sources of calcium may need to be considered.
Similar Questions
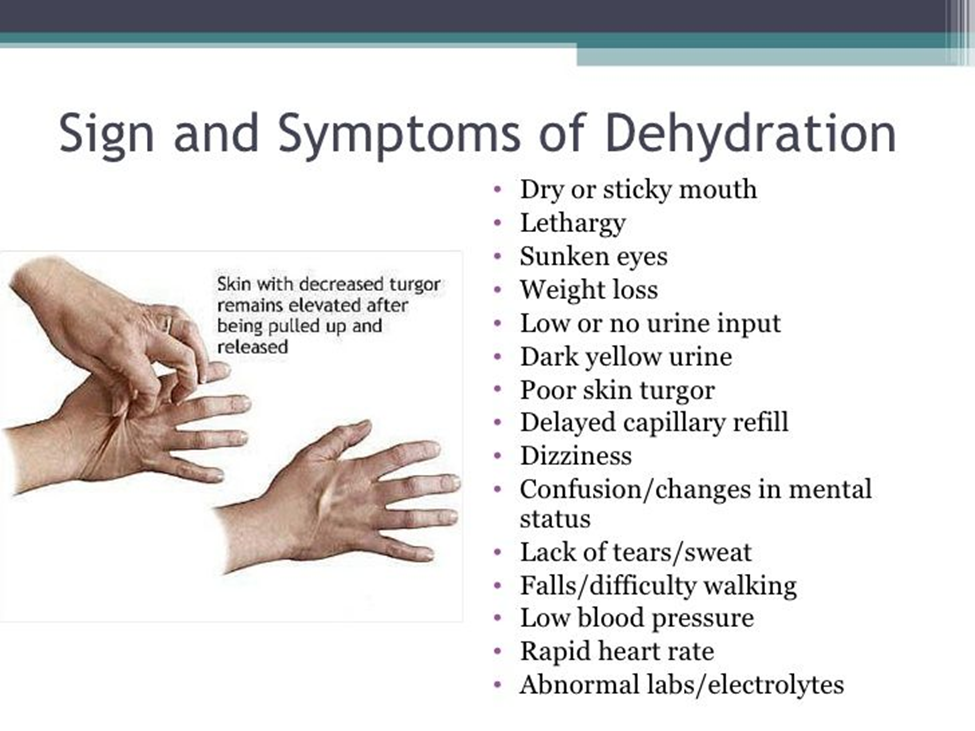
A nurse in a community clinic is collecting data from an older adult client who has a body mass index of 17.5. When evaluating the client for dehydration, the nurse should look for which of the following indications of fluid-volume deficit?
A. Tenting
TentingTenting refers to the delayed recoil of the skin when pinched. In a dehydrated state, the skin loses elasticity, leading to tenting due to decreased skin turgor. This is a specific sign of fluid-volume deficit.
B. Protruding eyeballs
Protruding eyeballsProtruding eyeballs are not typically associated with dehydration. This could be related to other conditions such as thyroid dysfunction, but it is not a specific indicator of fluid-volume deficit.
C. Elevated blood pressure
Elevated blood pressure Elevated blood pressure is not a typical sign of dehydration. In fact, dehydration often leads to a decrease in blood pressure due to reduced blood volume.
D. Dry mucous membranes
Dry mucous membranesDry mucous membranes can be an indication of dehydration, but in the context of the question, tenting (Option A) is a more specific sign related to skin turgor and is commonly assessed when evaluating for dehydration.
Full Explanation
A. Tenting
Tenting refers to the delayed recoil of the skin when pinched. In a dehydrated state, the skin loses elasticity, leading to tenting due to decreased skin turgor. This is a specific sign of fluid-volume deficit.
B. Protruding eyeballs
Protruding eyeballs are not typically associated with dehydration. This could be related to other conditions such as thyroid dysfunction, but it is not a specific indicator of fluid-volume deficit.
C. Elevated blood pressure
Elevated blood pressure is not a typical sign of dehydration. In fact, dehydration often leads to a decrease in blood pressure due to reduced blood volume.
D. Dry mucous membranes
Dry mucous membranes can be an indication of dehydration, but in the context of the question, tenting (Option A) is a more specific sign related to skin turgor and is commonly assessed when evaluating for dehydration.
A nurse is caring for a client who is in the oliguric phase of acute kidney injury. Which of the following actions should the nurse take?
A. Provide a diet high in protein.
Provide a diet high in protein.During the oliguric phase of acute kidney injury (AKI), there is a risk of electrolyte imbalances, including elevated levels of blood urea nitrogen (BUN) and creatinine. Restricting protein intake is often recommended during this phase to manage azotemia and prevent the accumulation of waste products that the kidneys may struggle to excrete.
B. Provide ibuprofen for retroperitoneal discomfort.
Provide ibuprofen for retroperitoneal discomfort.Ibuprofen and other nonsteroidal anti-inflammatory drugs (NSAIDs) are contraindicated in AKI. They can further compromise renal function and may contribute to acute tubular necrosis. NSAIDs can also affect renal blood flow, leading to worsening kidney function.
C. Monitor intake and output hourly
Monitor intake and output hourly. Monitoring intake and output (I&O) is a critical nursing intervention during the oliguric phase of AKI. Hourly monitoring helps assess renal function, fluid balance, and the effectiveness of interventions. It allows for early detection of changes that may require prompt intervention.
D. Encourage the client to consume at least 2 L of fluid daily
Encourage the client to consume at least 2 L of fluid daily.In the oliguric phase of AKI, fluid intake is often restricted to prevent fluid overload. Encouraging excessive fluid intake may contribute to fluid retention and worsen the oliguria. Fluid management is carefully regulated based on the individual client's needs and renal function.
Full Explanation
A. Provide a diet high in protein.
During the oliguric phase of acute kidney injury (AKI), there is a risk of electrolyte imbalances, including elevated levels of blood urea nitrogen (BUN) and creatinine. Restricting protein intake is often recommended during this phase to manage azotemia and prevent the accumulation of waste products that the kidneys may struggle to excrete.
B. Provide ibuprofen for retroperitoneal discomfort.
Ibuprofen and other nonsteroidal anti-inflammatory drugs (NSAIDs) are contraindicated in AKI. They can further compromise renal function and may contribute to acute tubular necrosis. NSAIDs can also affect renal blood flow, leading to worsening kidney function.
C. Monitor intake and output hourly.
Monitoring intake and output (I&O) is a critical nursing intervention during the oliguric phase of AKI. Hourly monitoring helps assess renal function, fluid balance, and the effectiveness of interventions. It allows for early detection of changes that may require prompt intervention.
D. Encourage the client to consume at least 2 L of fluid daily.
In the oliguric phase of AKI, fluid intake is often restricted to prevent fluid overload. Encouraging excessive fluid intake may contribute to fluid retention and worsen the oliguria. Fluid management is carefully regulated based on the individual client's needs and renal function.
Following admission, a client with a vascular occlusion of the right lower extremity calls the nurse and reports difficulty sleeping because of cold feet. Which of the following nursing actions should the nurse take to promote the client’s comfort?
A. Rub the client’s feet briskly for several minutes.
Rub the client’s feet briskly for several minutes.Rubbing the feet briskly may not be appropriate for a client with vascular occlusion. Vigorous rubbing could potentially cause damage to already compromised blood vessels, and the increased friction may not be well-tolerated.
B. Obtain a pair of slipper socks for the client.
Obtain a pair of slipper socks for the client.Providing slipper socks is a non-invasive and appropriate measure to help keep the client's feet warm. Slipper socks can offer comfort without the need for vigorous interventions or potential harm. They provide insulation and can be easily applied.
C. Increase the client’s oral fluid intake.
Increase the client’s oral fluid intake. While staying well-hydrated is generally important for overall health, increasing oral fluid intake may not directly address the specific issue of cold feet associated with vascular occlusion. It is essential to address the underlying circulatory issue causing the symptom.
D. Place a moist heating pad under the client’s feet.
Place a moist heating pad under the client’s feet.Applying heat, especially in the form of a moist heating pad, may not be recommended for a client with vascular occlusion. Heat can dilate blood vessels and potentially exacerbate the issue by increasing blood flow to the compromised extremity. It's important to avoid interventions that could worsen the vascular compromise.
Full Explanation
A. Rub the client’s feet briskly for several minutes.
Rubbing the feet briskly may not be appropriate for a client with vascular occlusion. Vigorous rubbing could potentially cause damage to already compromised blood vessels, and the increased friction may not be well-tolerated.
B. Obtain a pair of slipper socks for the client.
Providing slipper socks is a non-invasive and appropriate measure to help keep the client's feet warm. Slipper socks can offer comfort without the need for vigorous interventions or potential harm. They provide insulation and can be easily applied.
C. Increase the client’s oral fluid intake.
While staying well-hydrated is generally important for overall health, increasing oral fluid intake may not directly address the specific issue of cold feet associated with vascular occlusion. It is essential to address the underlying circulatory issue causing the symptom.
D. Place a moist heating pad under the client’s feet.
Applying heat, especially in the form of a moist heating pad, may not be recommended for a client with vascular occlusion. Heat can dilate blood vessels and potentially exacerbate the issue by increasing blood flow to the compromised extremity. It's important to avoid interventions that could worsen the vascular compromise.