Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
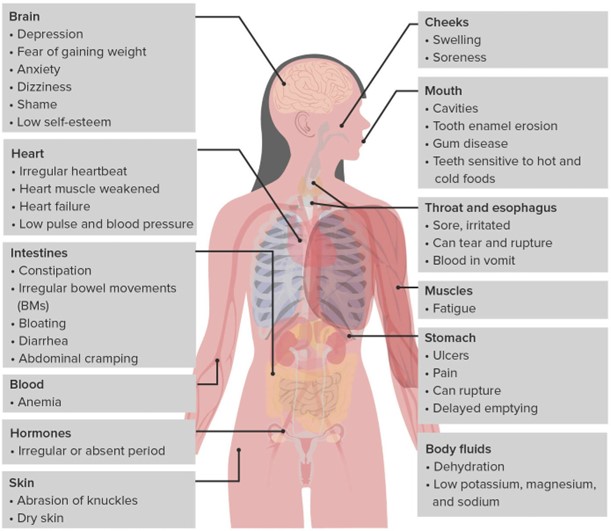
A nurse is reviewing the laboratory results of a client who has bulimia nervosa. The nurse should notify the provider of which of the following results?
A. Potassium 3.2 mEq/L
The nurse should notify the provider of the result indicating a low potassium level of 3.2 mEq/L in the client with bulimia nervosa. Low potassium levels, known as hypokalemia, can be a significant concern in individuals with bulimia nervosa due to the frequent purging behaviors associated with the condition. Purging, such as self-induced vomiting or misuse of laxatives or diuretics, can lead to excessive loss of potassium from the body. Hypokalemia can have serious consequences, including cardiac arrhythmias, muscle weakness, fatigue, and even life-threatening complications. The normal range for potassium is typically around 3.5-5.0 mEq/L. With a potassium level of 3.2 mEq/L falling below the normal range, it indicates a low potassium level and requires prompt attention.
B. WBC 5,200/mm3
A WBC (white blood cell) count of 5,200/mm3 falls within the normal range (typically between 4,500 and 11,000/mm3) and indicates a normal white blood cell count.
C. Hgb 14 g/dL
An Hgb (hemoglobin) level of 14 g/dL falls within the normal range (typically between 12 and 16 g/dL) and indicates a normal hemoglobin level.
D. Magnesium 1.6 mEq/L
A magnesium level of 1.6 mEq/L, although slightly low, is still within the normal range (typically between 1.5 and 2.5 mEq/L). The nurse should monitor it closely and assess for symptoms associated with hypomagnesemia. If the client's symptoms or other clinical indications suggest a significant magnesium imbalance, the healthcare provider should be notified.
This question is an excerpt from Nurse Dive's nursing test bank - ATI RN Nutrition 2019 Proctored Exam. Take the full exam now
Full Explanation
Low potassium levels, known as hypokalemia, can be a significant concern in individuals with bulimia nervosa due to the frequent purging behaviors associated with the condition. Purging, such as self-induced vomiting or misuse of laxatives or diuretics, can lead to excessive loss of potassium from the body. Hypokalemia can have serious consequences, including cardiac arrhythmias, muscle weakness, fatigue, and even life-threatening complications.
The normal range for potassium is typically around 3.5-5.0 mEq/L. With a potassium level of 3.2 mEq/L falling below the normal range, it indicates a low potassium level and requires prompt attention.
The other laboratory results mentioned in the question are within normal ranges:
● A WBC (white blood cell) count of 5,200/mm3 falls within the normal range (typically between 4,500 and 11,000/mm3) and indicates a normal white blood cell count.
● An Hgb (hemoglobin) level of 14 g/dL falls within the normal range (typically between 12 and 16 g/dL) and indicates a normal hemoglobin level.
● A magnesium level of 1.6 mEq/L, although slightly low, is still within the normal range (typically between 1.5 and 2.5 mEq/L). The nurse should monitor it closely and assess for symptoms associated with hypomagnesemia. If the client's symptoms or other clinical indications suggest a significant magnesium imbalance, the healthcare provider should be notified.
Similar Questions
A nurse is providing teaching to a client who has type 1 diabetes mellitus. Which of the following statements by the client indicates an understanding of the teaching?
A. "I will have ketones in my urine if my blood glucose is maintained at 190 milligrams per deciliter."
In type 1 diabetes mellitus, when blood glucose levels are consistently high, the body may start breaking down fat for energy, leading to the production of ketones. Ketones can be detected in urine as a result. A blood glucose level of 190 milligrams per deciliter is elevated and can potentially trigger the production of ketones. Monitoring urine for ketones can be an important indicator of diabetes management and helps identify potential complications.
B. "I will keep my blood glucose levels between 200 and 212 milligrams per deciliter."
"I will keep my blood glucose levels between 200 and 212 milligrams per deciliter": This statement suggests a target range that is higher than the recommended target blood glucose levels for individuals with diabetes. Generally, the target range for blood glucose levels in individuals with diabetes is lower, typically between 80-130 mg/dL before meals and below 180 mg/dL after meals.
C. "I will keep my HbA1c at five percent."
"I will keep my HbA1c at five percent": While maintaining a lower HbA1c level is generally desirable for individuals with diabetes, a target of five percent is too low. HbA1c is a measure of average blood glucose levels over the past two to three months. The American Diabetes Association (ADA) recommends an HbA1c target of less than 7 percent for most adults with diabetes, although individualized targets may vary based on factors such as age and other health conditions.
D. "Albumin in my urine is an indication of normal kidney function."
"Albumin in my urine is an indication of normal kidney function": This statement is incorrect. The presence of albumin in the urine, called albuminuria, is an indication of kidney damage or dysfunction. It is a common sign of kidney disease, including diabetic nephropathy, which is a complication of diabetes affecting the kidneys.
Full Explanation
In type 1 diabetes mellitus, when blood glucose levels are consistently high, the body may start breaking down fat for energy, leading to the production of ketones. Ketones can be detected in urine as a result. A blood glucose level of 190 milligrams per deciliter is elevated and can potentially trigger the production of ketones. Monitoring urine for ketones can be an important indicator of diabetes management and helps identify potential complications.
The other statements by the client indicate a lack of understanding or potential misconceptions:
● "I will keep my blood glucose levels between 200 and 212 milligrams per deciliter": This statement suggests a target range that is higher than the recommended target blood glucose levels for individuals with diabetes. Generally, the target range for blood glucose levels in individuals with diabetes is lower, typically between 80-130 mg/dL before meals and below 180 mg/dL after meals.
● "Albumin in my urine is an indication of normal kidney function": This statement is incorrect. The presence of albumin in the urine, called albuminuria, is an indication of kidney damage or dysfunction. It is a common sign of kidney disease, including diabetic nephropathy, which is a complication of diabetes affecting the kidneys.
● "I will keep my HbA1c at five percent": While maintaining a lower HbA1c level is generally desirable for individuals with diabetes, a target of five percent is too low. HbA1c is a measure of average blood glucose levels over the past two to three months. The American Diabetes Association (ADA) recommends an HbA1c target of less than 7 percent for most adults with diabetes, although individualized targets may vary based on factors such as age and other health conditions.
A nurse is teaching a client who reports wanting to lose weight about behavioral modifications. Which of the following statements should the nurse include in the teaching?
A. "Make sure to drink water with your meals."
According to some sources, behavioral modifications for weight loss include: Keeping a food journal to track your intake and identify patterns Eating smaller portions and using smaller plates Filling half of your plate with fruits and vegetables Getting plenty of sleep and drinking fluids Eating slowly and consciously Eating breakfast every day Avoiding high-calorie add-ons such as cream, butter, mayonnaise and salad dressings Not eating while watching television, reading, working or doing other activities Planning healthy snacks and meals in advance and bringing them to work Replacing eating with another activity that you will not associate with food Based on these suggestions, the statement that the nurse should include in the teaching is “Make sure to drink water with your meals.” This can help you feel full and hydrated, and reduce your calorie intake from other beverages.
B. "Your biggest meal of the day should be breakfast."
Your biggest meal of the day should be breakfast. This is not a behavioral modification, but a dietary recommendation that may vary depending on your preferences and needs.
C. "Meal replacement shakes can cause weight gain."
Meal replacement shakes can cause weight gain. This is not a behavioral modification, but a claim that is not supported by evidence. Meal replacement shakes can be part of a weight loss plan if they are used appropriately and provide adequate nutrition.
D. "Set your weight loss goal to 2.5 pounds per week."
Set your weight loss goal to 2.5 pounds per week. This is not a behavioral modification, but a goal that may be unrealistic or unhealthy for some people. A more reasonable goal is to lose 1 to 2 pounds per week.
Full Explanation
According to some sources, behavioral modifications for weight loss include:
● Keeping a food journal to track your intake and identify patterns
● Eating smaller portions and using smaller plates
● Filling half of your plate with fruits and vegetables
● Getting plenty of sleep and drinking fluids
● Eating slowly and consciously
● Eating breakfast every day
● Avoiding high-calorie add-ons such as cream, butter, mayonnaise and salad dressings
● Not eating while watching television, reading, working or doing other activities
● Planning healthy snacks and meals in advance and bringing them to work
● Replacing eating with another activity that you will not associate with food
Based on these suggestions, the statement that the nurse should include in the teaching is “Make sure to drink water with your meals.” This can help you feel full and hydrated, and reduce your calorie intake from other beverages.
The other statements are either false or not related to behavioral modifications. For example:
● Your biggest meal of the day should be breakfast. This is not a behavioral modification, but a dietary recommendation that may vary depending on your preferences and needs.
● Meal replacement shakes can cause weight gain. This is not a behavioral modification, but a claim that is not supported by evidence. Meal replacement shakes can be part of a weight loss plan if they are used appropriately and provide adequate nutrition.
● Set your weight loss goal to 2.5 pounds per week. This is not a behavioral modification, but a goal that may be unrealistic or unhealthy for some people. A more reasonable goal is to lose 1 to 2 pounds per week.
A nurse in a long-term care facility is implementing a nutrition plan for a client who is at risk for malnutrition. Which of the following actions should the nurse include in the plan? (Select all that apply.)
A. Assess for pain prior to mealtime.
Assess for pain prior to mealtime: Pain can significantly impact a person's appetite and ability to eat. Assessing for pain before mealtime can help identify any discomfort that may hinder the client's ability to eat.
B. Discourage snacks between meals.
Discourage snacks between meals: For clients at risk for malnutrition, it may be necessary to encourage nutrient-dense snacks between meals to increase caloric intake. Discouraging snacks may further contribute to malnutrition.
C. Provide mouth care before feeding.
Provide mouth care before feeding: Proper oral hygiene is essential for maintaining a healthy appetite and preventing oral health issues that can affect eating. Providing mouth care before feeding helps ensure a clean and comfortable oral environment.
D. Remove the bedpan from the client's sight.
Remove the bedpan from the client's sight: Sight and smell can have a significant impact on a person's appetite. Removing the bedpan from the client's sight can help create a more pleasant dining environment and promote a better appetite.
E. Administer antiemetics following the meal.
Administer antiemetics following the meal: Administering antiemetics following a meal is not a routine action in a nutrition plan. Antiemetics are typically used to treat nausea and vomiting, which may interfere with a person's ability to eat, but their administration should be based on specific symptoms and prescribed by a healthcare provider.
Full Explanation
In a nutrition plan for a client at risk for malnutrition, the nurse should include the following actions:
Assess for pain prior to mealtime: Pain can significantly impact a person's appetite and ability to eat. Assessing for pain before mealtime can help identify any discomfort that may hinder the client's ability to eat.
Provide mouth care before feeding: Proper oral hygiene is essential for maintaining a healthy appetite and preventing oral health issues that can affect eating. Providing mouth care before feeding helps ensure a clean and comfortable oral environment.
Remove the bedpan from the client's sight: Sight and smell can have a significant impact on a person's appetite. Removing the bedpan from the client's sight can help create a more pleasant dining environment and promote a better appetite.
However, the following actions should not be included in the plan:
Discourage snacks between meals: For clients at risk for malnutrition, it may be necessary to encourage nutrient-dense snacks between meals to increase caloric intake. Discouraging snacks may further contribute to malnutrition.
Administer antiemetics following the meal: Administering antiemetics following a meal is not a routine action in a nutrition plan. Antiemetics are typically used to treat nausea and vomiting, which may interfere with a person's ability to eat, but their administration should be based on specific symptoms and prescribed by a healthcare provider.