Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is verifying informed consent for a client who is preoperative for a vaginal hysterectomy. Which of the following statements should the nurse identify as an indication that the client has given informed consent?
A. “I will have a large scar on my stomach after this procedure."
This is incorrect for a vaginal hysterectomy, which does not involve an abdominal incision.
B. "I am thankful I am done having children."
'I am thankful I am done having children." This statement reflects an understanding of a key consequence of a hysterectomy, which is the removal of the uterus and the resulting inability to have children. This indicates that the client is aware of and accepts the major impact of the surgery on their reproductive capabilities.
C. "I should expect my periods to resume in 1 month."
"I should expect my periods to resume in 1 month.": This is incorrect because the removal of the uterus means the client will no longer have menstrual periods.
D. "I will no longer need a regular gynecological examination."
"I will no longer need a regular gynecological examination.": This is incorrect because regular gynecological examinations are still necessary to monitor overall reproductive health and screen for other conditions.
This question is an excerpt from Nurse Dive's nursing test bank - ATI PN Comprehensive Predictor 2023 - Proctored Exam 1. Take the full exam now
Full Explanation
Informed consent is a process where the healthcare provider explains the risks, benefits, and alternatives of a proposed procedure or treatment to the client. The client then demonstrates their understanding of this information and voluntarily agrees to undergo the procedure or treatment.
A. "I will have a large scar on my stomach after this procedure". This is incorrect for a vaginal hysterectomy, which does not involve an abdominal incision.
B. 'I am thankful I am done having children." This statement reflects an understanding of a key consequence of a hysterectomy, which is the removal of the uterus and the resulting inability to have children. This indicates that the client is aware of and accepts the major impact of the surgery on their reproductive capabilities.
C. "I should expect my periods to resume in 1 month.": This is incorrect because the removal of the uterus means the client will no longer have menstrual periods.
D. "I will no longer need a regular gynecological examination.": This is incorrect because regular gynecological examinations are still necessary to monitor overall reproductive health and screen for other conditions.
Similar Questions
A nurse is caring for a client who has an indwelling catheter with a urinary drainage system. Which of the following actions should the nurse take?
A. Coil the tubing on the bed above the collection bag.
Coiling the tubing on the bed above the collection bag is incorrect because it can cause urine to flow back into the bladder, increasing the risk of infection and compromising the effectiveness of the drainage system. The tubing should be kept below the level of the bladder to ensure proper drainage.
B. Instruct the client to hold the drainage bag at waist height when ambulating.
Instructing the client to hold the drainage bag at waist height when ambulating is incorrect because the drainage bag should always be kept below the level of the bladder to prevent urine from flowing back into the bladder, which could lead to a urinary tract infection (UTI).
C. Secure the tubing with adhesive tape to the lower abdomen.
Securing the tubing with adhesive tape to the lower abdomen is correct because it helps prevent accidental pulling or tugging on the catheter, which could cause discomfort or dislodgement. Properly securing the tubing also helps maintain a continuous flow of urine and reduces the risk of infection.
D. Collect a sterile specimen from the urinary drainage bag.
Collecting a sterile specimen from the urinary drainage bag is incorrect because urine in the drainage bag is not considered sterile. If a sterile specimen is needed, it should be obtained by cleaning the catheter's sampling port with an antiseptic solution and withdrawing urine directly from the port using a sterile syringe.
Full Explanation
A. Coiling the tubing on the bed above the collection bag is incorrect because it can cause urine to flow back into the bladder, increasing the risk of infection and compromising the effectiveness of the drainage system. The tubing should be kept below the level of the bladder to ensure proper drainage.
B. Instructing the client to hold the drainage bag at waist height when ambulating is incorrect because the drainage bag should always be kept below the level of the bladder to prevent urine from flowing back into the bladder, which could lead to a urinary tract infection (UTI).
C. Securing the tubing with adhesive tape to the lower abdomen is correct because it helps prevent accidental pulling or tugging on the catheter, which could cause discomfort or dislodgement. Properly securing the tubing also helps maintain a continuous flow of urine and reduces the risk of infection.
D. Collecting a sterile specimen from the urinary drainage bag is incorrect because urine in the drainage bag is not considered sterile. If a sterile specimen is needed, it should be obtained by cleaning the catheter's sampling port with an antiseptic solution and withdrawing urine directly from the port using a sterile syringe.
A nurse is collecting data for a client who is receiving enteral tube feedings. The nurse should identify that which of the following findings is a manifestation of fluid overload?
A. Weight loss
Weight loss is typically associated with inadequate calorie or nutrient intake, rather than fluid overload.
B. Decreased blood pressure
Weight loss is typically associated with inadequate calorie or nutrient intake, rather than fluid overload.
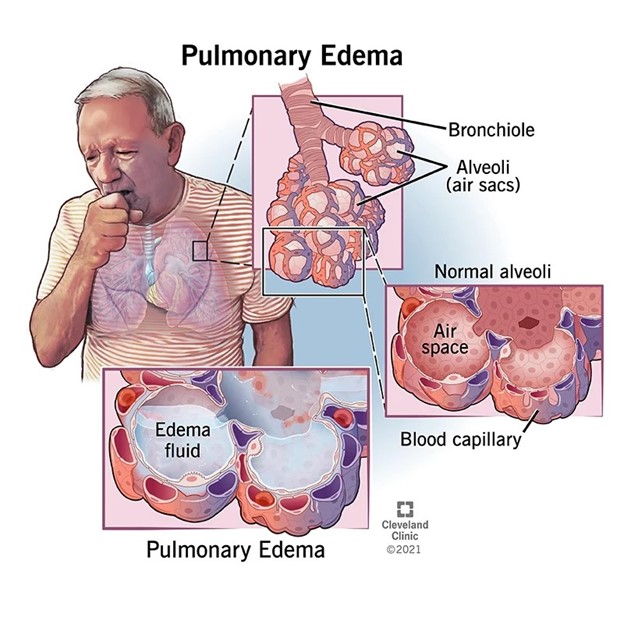
C. Crackles heard in the lungs
Fluid overload refers to an excess volume of fluid in the body, which can occur as a result of various factors, including excessive fluid intake or inadequate fluid removal. Crackles heard in the lungs, also known as rales, can indicate fluid accumulation in the lungs, a condition known as pulmonary edema. It is a common manifestation of fluid overload and can be detected through auscultation of the lungs.
D. Decreased skin turgor
Weight loss is typically associated with inadequate calorie or nutrient intake, rather than fluid overload.
Full Explanation
Fluid overload refers to an excess volume of fluid in the body, which can occur as a result of various factors, including excessive fluid intake or inadequate fluid removal. Crackles heard in the lungs, also known as rales, can indicate fluid accumulation in the lungs, a condition known as pulmonary edema. It is a common manifestation of fluid overload and can be detected through auscultation of the lungs.
Weight loss is typically associated with inadequate calorie or nutrient intake, rather than fluid overload.
Weight loss is typically associated with inadequate calorie or nutrient intake, rather than fluid overload.
Weight loss is typically associated with inadequate calorie or nutrient intake, rather than fluid overload.
A nurse is performing nasopharyngeal suctioning for an adult client. Which of the following techniques should the nurse use?
A. Apply suction while inserting the catheter.
This is incorrect because suction should not be applied during the insertion of the catheter. Suctioning should only be applied while withdrawing the catheter to avoid causing trauma to the mucosa.
B. Apply intermittent suction for 15 seconds.
Suctioning should generally be performed for no longer than 10 seconds at a time to minimize the risk of complications such as hypoxia.
C. Wait 1 min between suctioning attempts.
This response is correct because waiting approximately 1 minute between suctioning attempts allows the client time to recover and reoxygenate. This interval helps prevent hypoxia and mucosal damage, which are important considerations during the suctioning process.
D. Insert the catheter 10 cm (4 in).
In adults insert catheter approximately 16 cm (6.5 inches); in older children, 8– 12 cm (3–5 inches); in infants and young children, 4–7.5 cm (1.5–3 inches). Rule of thumb is to insert catheter distance from tip of nose (or mouth) to angle of mandible.
Full Explanation
A. This is incorrect because suction should not be applied during the insertion of the catheter. Suctioning should only be applied while withdrawing the catheter to avoid causing trauma to the mucosa.
B. Suctioning should generally be performed for no longer than 10 seconds at a time to minimize the risk of complications such as hypoxia.
C. This response is correct because waiting approximately 1 minute between suctioning attempts allows the client time to recover and reoxygenate. This interval helps prevent hypoxia and mucosal damage, which are important considerations during the suctioning process.
D. In adults insert catheter approximately 16 cm (6.5 inches); in older children, 8– 12 cm (3–5 inches); in infants and young children, 4–7.5 cm (1.5–3 inches). Rule of thumb is to insert catheter distance from tip of nose (or mouth) to angle of mandible.