Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse on the labor and delivery unit is caring for a client following a vaginal examination by the provider, which is documented as: 1/50%/-2. Which of the following interpretations of this finding should the nurse make?
A. The presenting part is 1 cm above the ischial spines.
Choice A reason: The presenting part is 1 cm above the ischial spines. This statement would be documented as -1 station. Fetal station is measured in centimeters relative to the ischial spines, with negative numbers indicating the presenting part is above the spines.
B. The cervix is effaced 1 cm.
Choice B reason: The cervix is effaced 1 cm. Effacement is measured in percentages, not centimeters. It refers to the thinning of the cervix, which progresses from 0% (not effaced) to 100% (fully effaced).
C. The cervix is 1 cm dilated.
Choice C reason: In obstetrics, a sterile vaginal exam (SVE) is recorded using a standard three-part shorthand: Dilation / Effacement / Station. Dilation: This is always the first number in the sequence. It measures the opening of the cervix from 0 to 10 centimeters. Therefore, if the finding begins with the number 1, it indicates the cervix has opened to a diameter of 1 cm.
D. The presenting part is 1 cm below the ischial spines.
Choice D reason: The presenting part is 1 cm below the ischial spines. This would be documented as +1 station. Positive numbers indicate the presenting part is below the ischial spines, moving towards delivery.
E. None
None
F. None
None
This question is an excerpt from Nurse Dive's nursing test bank - ATI Maternity Exam - Proctored Exam 2. Take the full exam now
Full Explanation
The correct answer is: c. The cervix is 1 cm dilated.
Choice A reason:
The presenting part is 1 cm above the ischial spines. This statement would be documented as -1 station. Fetal station is measured in centimeters relative to the ischial spines, with negative numbers indicating the presenting part is above the spines.
Choice B reason:
The cervix is effaced 1 cm. Effacement is measured in percentages, not centimeters. It refers to the thinning of the cervix, which progresses from 0% (not effaced) to 100% (fully effaced).
Choice C reason:
In obstetrics, a sterile vaginal exam (SVE) is recorded using a standard three-part shorthand: Dilation / Effacement / Station. Dilation: This is always the first number in the sequence. It measures the opening of the cervix from 0 to 10 centimeters. Therefore, if the finding begins with the number 1, it indicates the cervix has opened to a diameter of 1 cm.
Choice D reason:
The presenting part is 1 cm below the ischial spines. This would be documented as +1 station. Positive numbers indicate the presenting part is below the ischial spines, moving towards delivery.
Similar Questions
A nurse is admitting a client who is at 38 weeks of gestation and is in the active phase of the first stage of labor. Which of the following assessment findings is the first priority for the nurse to report to the provider?
A. Contractions lasting 2 minutes and with no rest between contractions.
The first priority assessment finding to report to the provider is contractions lasting 2 minutes and with no rest between contractions. Prolonged contractions without adequate rest can lead to uterine hyperstimulation and fetal distress, potentially compromising the wellbeing of both the client and the baby. The provider needs to be informed immediately for further evaluation and intervention.
B. Pressure on the perineum causing the client to have the desire to bear down.
Pressure on the perineum and the desire to bear down indicate that the client is experiencing the urge to push, which is expected during the second stage of labor, not during the active phase of the first stage. It is not the first priority to report.
C. Discharge consisting of clear fluid from the vagina.
Clear fluid discharge from the vagina can indicate rupture of membranes, but it is not an immediate concern unless the fluid is meconiumstained or there are other signs of fetal distress.
D. Passage of a bloodtinged mucous plug.
Passage of a bloodtinged mucous plug (also known as "bloody show") is a common sign that labor is approaching, but it is not an immediate concern unless there are other signs of labor progression or complications. It is not the first priority to report.
Full Explanation
Choice A: The first priority assessment finding to report to the provider is contractions lasting 2 minutes and with no rest between contractions. Prolonged contractions without adequate rest can lead to uterine hyperstimulation and fetal distress, potentially compromising the wellbeing of both the client and the baby. The provider needs to be informed immediately for further
evaluation and intervention.
Choice B: Pressure on the perineum and the desire to bear down indicate that the client is experiencing the urge to push, which is expected during the second stage of labor, not during the active phase of the first stage. It is not the first priority to report.
Choice C: Clear fluid discharge from the vagina can indicate rupture of membranes, but it is not an immediate concern unless the fluid is meconiumstained or there are other signs of fetal distress.
Choice D: Passage of a bloodtinged mucous plug (also known as "bloody show") is a common sign that labor is approaching, but it is not an immediate concern unless there are other signs of labor progression or complications. It is not the first priority to report.
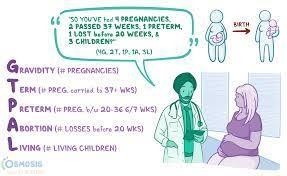
A nurse in a prenatal clinic is reviewing the health record of a client who is at 28 weeks of gestation. The history includes one pregnancy, terminated by elective abortion at 9 weeks; the birth of twins at 36 weeks; and a spontaneous abortion at 15 weeks. According to the GTPAL system, which of thea following describes the client's current status?
A. 40122
The GTPAL system is used to assess a client's obstetric history: G (Gravida): The total number of pregnancies, including the current one. T (Term births): The number of pregnancies carried to at least 37 weeks. P (Preterm births): The number of pregnancies delivered between 20 and 36 weeks, 6 days. A (Abortions): The number of pregnancies ending before 20 weeks (spontaneous or elective). L (Living children): The number of children currently alive. For this client: G (Gravida): 4 (one elective abortion, one twin pregnancy, one spontaneous abortion, and the current pregnancy). T (Term births): 0 (the twin pregnancy was delivered at 36 weeks, which is preterm). P (Preterm births): 1 (twins delivered at 36 weeks count as one preterm birth). A (Abortions): 2 (one elective abortion at 9 weeks, one spontaneous abortion at 15 weeks). L (Living children): 2 (the twins). Thus, the GTPAL for this client is 4-0-1-2-2.
B. 20020
The GTPAL system is used to assess a client's obstetric history: G (Gravida): The total number of pregnancies, including the current one. T (Term births): The number of pregnancies carried to at least 37 weeks. P (Preterm births): The number of pregnancies delivered between 20 and 36 weeks, 6 days. A (Abortions): The number of pregnancies ending before 20 weeks (spontaneous or elective). L (Living children): The number of children currently alive. For this client: G (Gravida): 4 (one elective abortion, one twin pregnancy, one spontaneous abortion, and the current pregnancy). T (Term births): 0 (the twin pregnancy was delivered at 36 weeks, which is preterm). P (Preterm births): 1 (twins delivered at 36 weeks count as one preterm birth). A (Abortions): 2 (one elective abortion at 9 weeks, one spontaneous abortion at 15 weeks). L (Living children): 2 (the twins). Thus, the GTPAL for this client is 4-0-1-2-2.
C. 40122
The GTPAL system is used to assess a client's obstetric history: G (Gravida): The total number of pregnancies, including the current one. T (Term births): The number of pregnancies carried to at least 37 weeks. P (Preterm births): The number of pregnancies delivered between 20 and 36 weeks, 6 days. A (Abortions): The number of pregnancies ending before 20 weeks (spontaneous or elective). L (Living children): The number of children currently alive. For this client: G (Gravida): 4 (one elective abortion, one twin pregnancy, one spontaneous abortion, and the current pregnancy). T (Term births): 0 (the twin pregnancy was delivered at 36 weeks, which is preterm). P (Preterm births): 1 (twins delivered at 36 weeks count as one preterm birth). A (Abortions): 2 (one elective abortion at 9 weeks, one spontaneous abortion at 15 weeks). L (Living children): 2 (the twins). Thus, the GTPAL for this client is 4-0-1-2-2.
D. 30202
The GTPAL system is used to assess a client's obstetric history: G (Gravida): The total number of pregnancies, including the current one. T (Term births): The number of pregnancies carried to at least 37 weeks. P (Preterm births): The number of pregnancies delivered between 20 and 36 weeks, 6 days. A (Abortions): The number of pregnancies ending before 20 weeks (spontaneous or elective). L (Living children): The number of children currently alive. For this client: G (Gravida): 4 (one elective abortion, one twin pregnancy, one spontaneous abortion, and the current pregnancy). T (Term births): 0 (the twin pregnancy was delivered at 36 weeks, which is preterm). P (Preterm births): 1 (twins delivered at 36 weeks count as one preterm birth). A (Abortions): 2 (one elective abortion at 9 weeks, one spontaneous abortion at 15 weeks). L (Living children): 2 (the twins). Thus, the GTPAL for this client is 4-0-1-2-2.
E. None
None
F. None
None
Full Explanation
The correct answer is: c. 42022
Choice A: 40122
Reason: This choice is incorrect because it indicates 4 pregnancies (correct), 0 term births (correct), 1 preterm birth (correct), 2 abortions (correct), but 2 living children (incorrect). The client has 2 living children, which is correct, but the term and preterm counts are not accurate.
Choice B: 20020
Reason: This choice is incorrect because it indicates 2 pregnancies (incorrect), 0 term births (correct), 0 preterm births (incorrect), 2 abortions (correct), and 0 living children (incorrect). The client has had 4 pregnancies, 1 preterm birth, and 2 living children.
Choice C: 42022
Reason: This choice is correct. It indicates 4 pregnancies (current pregnancy, elective abortion, twins, spontaneous abortion), 0 term births, 2 preterm births (twins at 36 weeks), 2 abortions (elective at 9 weeks, spontaneous at 15 weeks), and 2 living children (twins).
Choice D:
The GTPAL system is used to assess a client's obstetric history:
- G (Gravida): The total number of pregnancies, including the current one.
- T (Term births): The number of pregnancies carried to at least 37 weeks.
- P (Preterm births): The number of pregnancies delivered between 20 and 36 weeks, 6 days.
- A (Abortions): The number of pregnancies ending before 20 weeks (spontaneous or elective).
- L (Living children): The number of children currently alive.
For this client:
G (Gravida): 4 (one elective abortion, one twin pregnancy, one spontaneous abortion, and the current pregnancy).
- T (Term births): 0 (the twin pregnancy was delivered at 36 weeks, which is preterm).
- P (Preterm births): 1 (twins delivered at 36 weeks count as one preterm birth).
- A (Abortions): 2 (one elective abortion at 9 weeks, one spontaneous abortion at 15 weeks).
- L (Living children): 2 (the twins).
Thus, the GTPAL for this client is 4-0-1-2-2.
A nurse is assessing a client who is in the third trimester of pregnancy. The nurse should recognize which of the following findings as an expected physiologic change during pregnancy?
A. Posterior neck flexion
Posterior neck flexion is not an expected change during pregnancy.
B. Increased abdominal muscle tone
Increased abdominal muscle tone is not an expected change during pregnancy. In fact, the abdominal muscles tend to stretch and may become less toned as the uterus expands.
C. Gradual lordosis
During pregnancy, the woman's center of gravity shifts due to the growing uterus, leading to an increased arch in the lower back known as lordosis. This change helps to maintain balance and reduce the strain on the back. The other options are not expected physiologic changes during pregnancy.
D. Decreased mobility of pelvic joints
Decreased mobility of pelvic joints is not an expected change during pregnancy. Some joint laxity may occur due to hormonal changes, but decreased mobility is not typical.
Full Explanation
Choice A: Posterior neck flexion is not an expected change during pregnancy.
Choice B: Increased abdominal muscle tone is not an expected change during pregnancy. In fact, the abdominal muscles tend to stretch and may become less toned as the uterus expands.
Choice C: During pregnancy, the woman's center of gravity shifts due to the growing uterus, leading to an increased arch in the lower back known as lordosis. This change helps to maintain balance and reduce the strain on the back. The other options are not expected physiologic changes during pregnancy.
Choice D: Decreased mobility of pelvic joints is not an expected change during pregnancy. Some joint laxity may occur due to hormonal changes, but decreased mobility is not typical.