Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse working for a home health agency is assessing an older adult male client. Which of the following findings is the priority for the nurse to address?
A. Urinary hesitancy
Reason: This choice is incorrect because urinary hesitancy is not the priority finding for the nurse to address. Urinary hesitancy is a difficulty or delay in starting or maintaining a urine stream. It may be caused by various factors such as prostate enlargement, urinary tract infection, medication side effects, or psychological issues. It may cause discomfort, pain, or urinary retention, but it does not pose an immediate threat to the client's life.
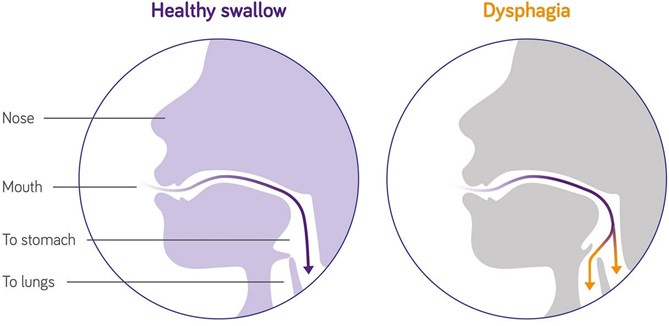
B. Dysphagia
Reason: This choice is correct because dysphagia is the priority finding for the nurse to address. Dysphagia is a difficulty or inability to swallow food or liquids. It may be caused by various factors such as stroke, Parkinson's disease, dementia, esophageal cancer, or oral infections. It may cause malnutrition, dehydration, aspiration, or choking, which can lead to serious complications such as pneumonia, sepsis, or death. Therefore, the nurse should assess the client's swallowing function and provide appropriate interventions such as modifying the diet texture, using thickening agents, or teaching swallowing techniques.
C. Swollen gums
Reason: This choice is incorrect because swollen gums are not the priority finding for the nurse to address. Swollen gums are an inflammation or enlargement of the gingival tissue that surrounds the teeth. They may be caused by various factors such as poor oral hygiene, gum disease, vitamin deficiency, medication side effects, or hormonal changes. They may cause bleeding, pain, or infection, but they do not pose an immediate threat to the client's life.
D. Pruritus
Reason: This choice is incorrect because pruritus is not the priority finding for the nurse to address. Pruritus is a sensation of itching that affects the skin. It may be caused by various factors such as dry skin, allergies, eczema, psoriasis, liver disease, or kidney disease. It may cause discomfort, scratching, or skin damage, but it does not pose an immediate threat to the client's life.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Custom N235 Final Summer 2023 Proctored Exam. Take the full exam now
Full Explanation
Choice A Reason: This choice is incorrect because urinary hesitancy is not the priority finding for the nurse to address.
Urinary hesitancy is a difficulty or delay in starting or maintaining a urine stream. It may be caused by various factors such as prostate enlargement, urinary tract infection, medication side effects, or psychological issues. It may cause discomfort, pain, or urinary retention, but it does not pose an immediate threat to the client's life.
Choice B Reason: This choice is correct because dysphagia is the priority finding for the nurse to address. Dysphagia is a difficulty or inability to swallow food or liquids. It may be caused by various factors such as stroke, Parkinson's disease, dementia, esophageal cancer, or oral infections. It may cause malnutrition, dehydration, aspiration, or choking, which can lead to serious complications such as pneumonia, sepsis, or death. Therefore, the nurse should assess the client's swallowing function and provide appropriate interventions such as modifying the diet texture, using thickening agents, or teaching swallowing techniques.
Choice C Reason: This choice is incorrect because swollen gums are not the priority finding for the nurse to address. Swollen gums are an inflammation or enlargement of the gingival tissue that surrounds the teeth. They may be caused by various factors such as poor oral hygiene, gum disease, vitamin deficiency, medication side effects, or hormonal changes. They may cause bleeding, pain, or infection, but they do not pose an immediate threat to the client's life.
Choice D Reason: This choice is incorrect because pruritus is not the priority finding for the nurse to address. Pruritus is a sensation of itching that affects the skin. It may be caused by various factors such as dry skin, allergies, eczema, psoriasis, liver disease, or kidney disease. It may cause discomfort, scratching, or skin damage, but it does not pose an immediate threat to the client's life.
Similar Questions
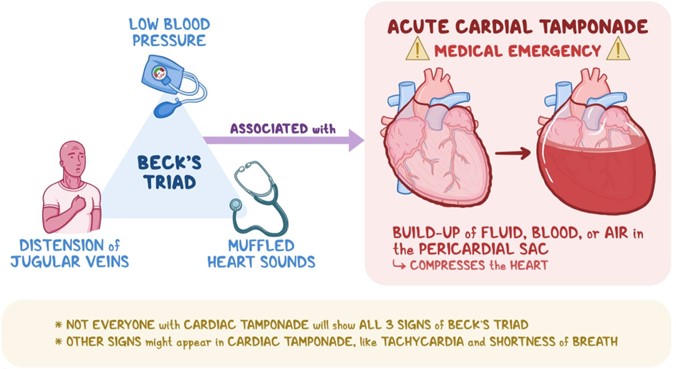
A nurse in a critical care unit is caring for a client who suffered a knife wound to the chest. The nurse suspects the client is developing cardiac tamponade. Which of the following assessment findings should the nurse identify as supporting this suspicion?
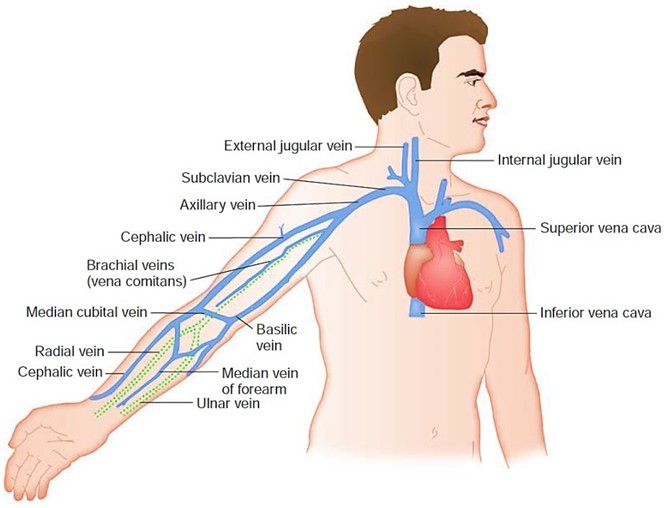
A. Flatened neck veins.
Reason: This choice is incorrect because flatened neck veins are not a sign of cardiac tamponade. Cardiac tamponade is a condition in which fluid accumulates in the pericardial sac that surrounds the heart, causing compression and impaired filling of the heart chambers. This leads to reduced cardiac output and hypotension. One of the manifestations of cardiac tamponade is distended neck veins due to increased venous pressure and impaired venous return.
B. Bradycardia.
Reason: This choice is incorrect because bradycardia is not a sign of cardiac tamponade. Bradycardia is a condition in which the heart rate is slower than normal (less than 60 beats per minute). It may be caused by various factors such as vagal stimulation, medication side effects, hypothyroidism, or sinus node dysfunction. It may cause symptoms such as fatigue, dizziness, or syncope, but it does not indicate cardiac tamponade.
C. Sudden lethargy.
Reason: This choice is incorrect because sudden lethargy is not a specific sign of cardiac tamponade. Lethargy is a condition in which the person feels tired, sluggish, or drowsy. It may be caused by various factors such as sleep deprivation, depression, infection, anemia, or hypoglycemia. It may affect the person's mental and physical performance, but it does not indicate cardiac tamponade.
D. Muffled heart sounds.
Reason: This choice is correct because muffled heart sounds are a sign of cardiac tamponade. Muffled heart sounds are heart sounds that are fainter or softer than normal due to reduced transmission of sound waves through fluid-filled pericardial sac. They may indicate that the heart function is compromised by cardiac tamponade and require immediate intervention such as pericardiocentesis (removal of fluid from pericardial sac).
Full Explanation
Choice A Reason: This choice is incorrect because flatened neck veins are not a sign of cardiac tamponade. Cardiac tamponade is a condition in which fluid accumulates in the pericardial sac that surrounds the heart, causing compression and impaired filling of the heart chambers. This leads to reduced cardiac output and hypotension. One of the manifestations of cardiac tamponade is distended neck veins due to increased venous pressure and impaired venous return.
Choice B Reason: This choice is incorrect because bradycardia is not a sign of cardiac tamponade. Bradycardia is a condition in which the heart rate is slower than normal (less than 60 beats per minute). It may be caused by various factors such as vagal stimulation, medication side effects, hypothyroidism, or sinus node dysfunction. It may cause symptoms such as fatigue, dizziness, or syncope, but it does not indicate cardiac tamponade.
Choice C Reason: This choice is incorrect because sudden lethargy is not a specific sign of cardiac tamponade. Lethargy is a condition in which the person feels tired, sluggish, or drowsy. It may be caused by various factors such as sleep deprivation, depression, infection, anemia, or hypoglycemia. It may affect the person's mental and physical performance, but it does not indicate cardiac tamponade.
Choice D Reason: This choice is correct because muffled heart sounds are a sign of cardiac tamponade. Muffled heart sounds are heart sounds that are fainter or softer than normal due to reduced transmission of sound waves through fluid-filled pericardial sac. They may indicate that the heart function is compromised by cardiac tamponade and require immediate intervention such as pericardiocentesis (removal of fluid from pericardial sac).
Here is the edited text:
A nurse is caring for a client who has a traumatic brain injury. The nurse notes that the client has a widening pulse pressure. Which of the following actions should the nurse take?
A. Administer a vasodilator medication.
Reason: This choice is incorrect because administering a vasodilator medication may lower the blood pressure and worsen the cerebral perfusion. A vasodilator medication is a drug that relaxes the blood vessels and reduces the resistance to blood flow. It may be used for clients who have hypertension, angina, or heart failure, but it does not help to reduce the intracranial pressure (ICP).
B. Elevate the head of the bed to 30°.
Reason: This choice is correct because elevating the head of the bed to 30° may help to improve the venous drainage and decrease the ICP. ICP is the pressure exerted by the brain tissue, cerebrospinal fluid (CSF), and blood within the cranial cavity. A normal ICP range is 5 to 15 mm Hg, and an elevated ICP (>20 mm Hg) can cause cerebral ischemia, herniation, or death. Therefore, positioning the client in a semi-Fowler's position (30° angle) or high- Fowler's position (60° to 90° angle) can facilitate breathing and prevent further complications.
C. Apply a cold compress to the forehead.
Reason: This choice is incorrect because applying a cold compress to the forehead may cause vasoconstriction and increase the ICP. A cold compress is a device that applies cold temperature to a body part to reduce inflammation, pain, or swelling. It may be used for clients who have headaches, sprains, or bruises, but it does not help to reduce the ICP.
D. Decrease the oxygen flow rate.
Reason: This choice is incorrect because decreasing the oxygen flow rate may cause hypoxia and worsen the cerebral ischemia. Hypoxia is a condition in which the body or a part of it does not receive enough oxygen. It may cause symptoms such as confusion, agitation, or cyanosis. Therefore, providing adequate oxygenation and ventilation is essential to maintain the brain function and prevent further damage.
Full Explanation
Choice A Reason: This choice is incorrect because administering a vasodilator medication may lower the blood pressure and worsen the cerebral perfusion. A vasodilator medication is a drug that relaxes the blood vessels and reduces the resistance to blood flow. It may be used for clients who have hypertension, angina, or heart failure, but it does not help to reduce the intracranial pressure (ICP).
Choice B Reason: This choice is correct because elevating the head of the bed to 30° may help to improve the venous drainage and decrease the ICP. ICP is the pressure exerted by the brain tissue, cerebrospinal fluid (CSF), and blood within the cranial cavity. A normal ICP range is 5 to 15 mm Hg, and an elevated ICP (>20 mm Hg) can cause cerebral ischemia, herniation, or death. Therefore, positioning the client in a semi-Fowler's position (30° angle) or high- Fowler's position (60° to 90° angle) can facilitate breathing and prevent further complications.
Choice C Reason: This choice is incorrect because applying a cold compress to the forehead may cause vasoconstriction and increase the ICP. A cold compress is a device that applies cold temperature to a body part to reduce inflammation, pain, or swelling. It may be used for clients who have headaches, sprains, or bruises, but it does not help to reduce the ICP.
Choice D Reason: This choice is incorrect because decreasing the oxygen flow rate may cause hypoxia and worsen the cerebral ischemia. Hypoxia is a condition in which the body or a part of it does not receive enough oxygen. It may cause symptoms such as confusion, agitation, or cyanosis. Therefore, providing adequate oxygenation and ventilation is essential to maintain the brain function and prevent further damage.
A nurse is assessing a client in the oliguric phase of acute kidney injury. Which of the following findings should the nurse expect?
A. Hypomagnesemia
Reason: This choice is incorrect because hypomagnesemia is not a common finding in the oliguric phase of acute kidney injury. Hypomagnesemia is a condition in which the serum magnesium level is lower than normal (less than 1.5 mEq/L). It may be caused by various factors such as malnutrition, diarrhea, diuretics, or alcohol abuse. It may cause symptoms such as muscle weakness, tremors, tetany, or cardiac arrhythmias.
B. Hyperkalemia
Reason: This choice is correct because hyperkalemia is a common finding in the oliguric phase of acute kidney injury. Hyperkalemia is a condition in which the serum potassium level is higher than normal (more than 5 mEq/L). It may be caused by reduced renal excretion of potassium due to decreased urine output (oliguria). It may cause symptoms such as muscle weakness, paresthesia, bradycardia, or cardiac arrest.
C. Decreased creatinine level
Reason: This choice is incorrect because decreased creatinine level is not a common finding in the oliguric phase of acute kidney injury. Creatinine is a waste product of muscle metabolism that is filtered by the kidneys and excreted in urine. A normal creatinine level ranges from 0.6 to 1.2 mg/dL for men and 0.5 to 1.1 mg/dL for women. In acute kidney injury, creatinine level usually increases due to reduced renal function and impaired clearance of creatinine.
D. Increased glomerular filtration rate (GFR)
Reason: This choice is incorrect because increased glomerular filtration rate (GFR) is not a common finding in the oliguric phase of acute kidney injury. GFR is a measure of how well the kidneys filter blood and remove waste products. A normal GFR range is 90,to 120 mL/min/1.73 m2. In acute kidney injury, GFR usually decreases due to reduced blood flow,to,the kidneys or damage to the glomeruli, which are the tiny blood vessels that filter blood in the kidneys.
Full Explanation
Choice A Reason: This choice is incorrect because hypomagnesemia is not a common finding in the oliguric phase of acute kidney injury. Hypomagnesemia is a condition in which the serum magnesium level is lower than normal (less than 1.5 mEq/L). It may be caused by various factors such as malnutrition, diarrhea, diuretics, or alcohol abuse. It may cause symptoms such as muscle weakness, tremors, tetany, or cardiac arrhythmias.
Choice B Reason: This choice is correct because hyperkalemia is a common finding in the oliguric phase of acute kidney injury. Hyperkalemia is a condition in which the serum potassium level is higher than normal (more than 5 mEq/L). It may be caused by reduced renal excretion of potassium due to decreased urine output (oliguria). It may cause symptoms such as muscle weakness, paresthesia, bradycardia, or cardiac arrest.
Choice C Reason: This choice is incorrect because decreased creatinine level is not a common finding in the oliguric phase of acute kidney injury. Creatinine is a waste product of muscle metabolism that is filtered by the kidneys and excreted in urine. A normal creatinine level ranges from 0.6 to 1.2 mg/dL for men and 0.5 to 1.1 mg/dL for women. In acute kidney injury, creatinine level usually increases due to reduced renal function and impaired clearance of creatinine.
Choice D Reason: This choice is incorrect because increased glomerular filtration rate (GFR) is not a common finding in the oliguric phase of acute kidney injury. GFR is a measure of how well
the kidneys filter blood and remove waste products.
A normal GFR range is 90,to 120 mL/min/1.73 m2. In acute kidney injury, GFR usually decreases due to reduced blood flow,to,the kidneys or damage to the glomeruli, which are the tiny blood vessels that filter blood in the kidneys.