Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A pregnant woman is admitted with premature rupture of the membranes. The nurse is assessing the woman closely for possible infection. Which findings would lead the nurse to suspect that the woman is developing an infection? Select all that apply.
A. Cloudy malodorous fluid
Choice A Reason: This is correct because cloudy malodorous fluid indicates that the amniotic fluid is contaminated with bacteria or other microorganisms that can cause infection in the woman or the fetus. Normally, amniotic fluid is clear and odorless.
B. Abdominal tenderness
Choice B Reason: This is correct because abdominal tenderness suggests that the woman has inflammation or irritation of the uterus or other pelvic organs due to infection. Abdominal tenderness can also be accompanied by cramping, pain, or fever.
C. Fetal bradycardia
Choice C Reason: This is correct because fetal bradycardia, which is a slow fetal heart rate below 110 beats per minute, indicates that the fetus is experiencing distress or hypoxia due to infection. Fetal bradycardia can be detected by electronic fetal monitoring or Doppler device.
D. Elevated maternal pulse rate
Choice D Reason: This is correct because elevated maternal pulse rate, which is a heart rate above 100 beats per minute, indicates that the woman has an increased metabolic demand or systemic inflammation due to infection. Elevated maternal pulse rate can also be caused by dehydration, anxiety, or pain.
E. Decreased C-reactive protein levels
Choice E Reason: This is incorrect because decreased C-reactive protein levels do not indicate infection. C-reactive protein (CRP) is a protein that is produced by the liver in response to inflammation or infection. Increased CRP levels can be a sign of infection, but decreased CRP levels can be normal or indicate other conditions such as liver disease or malnutrition.
This question is an excerpt from Nurse Dive's nursing test bank - Ati Maternal Newborn 4 Proctored Exam. Take the full exam now
Full Explanation
Choice A Reason: This is correct because cloudy malodorous fluid indicates that the amniotic fluid is contaminated with bacteria or other microorganisms that can cause infection in the woman or the fetus. Normally, amniotic fluid is clear and odorless.
Choice B Reason: This is correct because abdominal tenderness suggests that the woman has inflammation or irritation of the uterus or other pelvic organs due to infection. Abdominal tenderness can also be accompanied by cramping, pain, or fever.
Choice C Reason: This is correct because fetal bradycardia, which is a slow fetal heart rate below 110 beats per minute, indicates that the fetus is experiencing distress or hypoxia due to infection. Fetal bradycardia can be detected by electronic fetal monitoring or Doppler device.
Choice D Reason: This is correct because elevated maternal pulse rate, which is a heart rate above 100 beats per minute, indicates that the woman has an increased metabolic demand or systemic inflammation due to infection. Elevated maternal pulse rate can also be caused by dehydration, anxiety, or pain.
Choice E Reason: This is incorrect because decreased C-reactive protein levels do not indicate infection. C-reactive protein (CRP) is a protein that is produced by the liver in response to inflammation or infection. Increased CRP levels can be a sign of infection, but decreased CRP levels can be normal or indicate other conditions such as liver disease or malnutrition.
Similar Questions
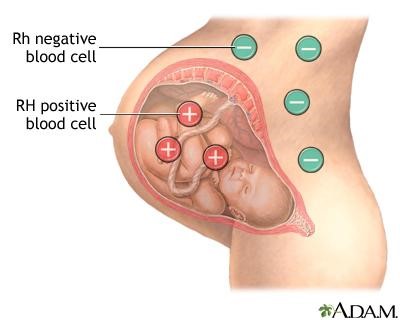
It is determined that a client's blood Rh is negative and her partner's is positive. To help prevent Rh isoimmunization, the nurse would expect to administer Rho(D) immune globulin at which time?
A. 24 hours before delivery and 24 hours after delivery
Reason: This is incorrect because administering Rho(D) immune globulin 24 hours before delivery is too early and may not provide adequate protection for the fetus. Administering it 24 hours after delivery is too late and may not prevent the mother from developing antibodies against the fetal Rh-positive blood cells.
B. In the first trimester and within 2 hours of delivery
Reason: This is incorrect because administering Rho(D) immune globulin in the first trimester is unnecessary and may not be effective, as the risk of Rh isoimmunization is very low before 28 weeks of gestation. Administering it within 2 hours of delivery is appropriate, but not sufficient, as it should be repeated within 72 hours after delivery.
C. At 28 weeks gestation and again within 72 hours after delivery
Reason: This is correct because administering Rho(D) immune globulin at 28 weeks gestation and again within 72 hours after delivery is the recommended schedule for preventing Rh isoimmunization in Rh-negative pregnant women who have Rh-positive partners. This regimen can prevent up to 99% of cases of Rh isoimmunization by blocking the maternal immune response to the fetal Rh-positive blood cells.
D. At 32 weeks gestation and immediately before discharge
Reason: This is incorrect because administering Rho(D) immune globulin at 32 weeks gestation is too late and may not prevent Rh isoimmunization if there has been any fetal-maternal hemorrhage before that time. Administering it immediately before discharge is also too late and may not prevent the mother from developing antibodies against the fetal Rh-positive blood cells.
Full Explanation
Choice A Reason: This is incorrect because administering Rho(D) immune globulin 24 hours before delivery is too early and may not provide adequate protection for the fetus. Administering it 24 hours after delivery is too late and may not prevent the mother from developing antibodies against the fetal Rh-positive blood cells.
Choice B Reason: This is incorrect because administering Rho(D) immune globulin in the first trimester is unnecessary and may not be effective, as the risk of Rh isoimmunization is very low before 28 weeks of gestation. Administering it within 2 hours of delivery is appropriate, but not sufficient, as it should be repeated within 72 hours after delivery.
Choice C Reason: This is correct because administering Rho(D) immune globulin at 28 weeks gestation and again within 72 hours after delivery is the recommended schedule for preventing Rh isoimmunization in Rh-negative pregnant women who have Rh-positive partners. This regimen can prevent up to 99% of cases of Rh isoimmunization by blocking the maternal immune response to the fetal Rh-positive blood cells.
Choice D Reason: This is incorrect because administering Rho(D) immune globulin at 32 weeks gestation is too late and may not prevent Rh isoimmunization if there has been any fetal-maternal hemorrhage before that time. Administering it immediately before discharge is also too late and may not prevent the mother from developing antibodies against the fetal Rh-positive blood cells.
It is determined that a client's blood Rh is negative and her partner's is positive. To help prevent Rh isoimmunization, the nurse would expect to administer Rho(D) immune globulin at which time?
A. 24 hours before delivery and 24 hours after delivery
Reason: This is incorrect because administering Rho(D) immune globulin 24 hours before delivery is too early and may not provide adequate protection for the fetus. Administering it 24 hours after delivery is too late and may not prevent the mother from developing antibodies against the fetal Rh-positive blood cells.
B. In the first trimester and within 2 hours of delivery
Reason: This is incorrect because administering Rho(D) immune globulin in the first trimester is unnecessary and may not be effective, as the risk of Rh isoimmunization is very low before 28 weeks of gestation. Administering it within 2 hours of delivery is appropriate, but not sufficient, as it should be repeated within 72 hours after delivery.
C. At 28 weeks gestation and again within 72 hours after delivery
Reason: This is correct because administering Rho(D) immune globulin at 28 weeks gestation and again within 72 hours after delivery is the recommended schedule for preventing Rh isoimmunization in Rh-negative pregnant women who have Rh-positive partners. This regimen can prevent up to 99% of cases of Rh isoimmunization by blocking the maternal immune response to the fetal Rh-positive blood cells.
D. At 32 weeks gestation and immediately before discharge
Reason: This is incorrect because administering Rho(D) immune globulin at 32 weeks gestation is too late and may not prevent Rh isoimmunization if there has been any fetal-maternal hemorrhage before that time. Administering it immediately before discharge is also too late and may not prevent the mother from developing antibodies against the fetal Rh-positive blood cells.
Full Explanation
Choice A Reason: This is incorrect because administering Rho(D) immune globulin 24 hours before delivery is too early and may not provide adequate protection for the fetus. Administering it 24 hours after delivery is too late and may not prevent the mother from developing antibodies against the fetal Rh-positive blood cells.
Choice B Reason: This is incorrect because administering Rho(D) immune globulin in the first trimester is unnecessary and may not be effective, as the risk of Rh isoimmunization is very low before 28 weeks of gestation. Administering it within 2 hours of delivery is appropriate, but not sufficient, as it should be repeated within 72 hours after delivery.
Choice C Reason: This is correct because administering Rho(D) immune globulin at 28 weeks gestation and again within 72 hours after delivery is the recommended schedule for preventing Rh isoimmunization in Rh-negative pregnant women who have Rh-positive partners. This regimen can prevent up to 99% of cases of Rh isoimmunization by blocking the maternal immune response to the fetal Rh-positive blood cells.
Choice D Reason: This is incorrect because administering Rho(D) immune globulin at 32 weeks gestation is too late and may not prevent Rh isoimmunization if there has been any fetal-maternal hemorrhage before that time. Administering it immediately before discharge is also too late and may not prevent the mother from developing antibodies against the fetal Rh-positive blood cells.
A client is diagnosed with gestational hypertension and is receiving magnesium sulfate. Which finding would the nurse interpret as indicating a therapeutic level of medication?
A. Difficulty in arousing
Reason: This is incorrect because difficulty in arousing is a sign of magnesium toxicity, which is a serious complication of magnesium sulfate therapy. Magnesium toxicity can cause central nervous system depression, muscle weakness, and cardiac arrest. The nurse should monitor the client's level of consciousness and stop the infusion if the client becomes lethargic or unresponsive.
B. Deep tendon reflexes 2+
Reason: This is correct because deep tendon reflexes 2+ indicate a normal and expected response to magnesium sulfate therapy. Magnesium sulfate is a muscle relaxant that can reduce the risk of seizures in gestational hypertension. The nurse should assess the client's deep tendon reflexes regularly and maintain them at 2+ or slightly diminished.
C. Urinary output of 30 mL per hour
Reason: This is incorrect because urinary output of 30 mL per hour is below the normal range of 40 to 80 mL per hour and may indicate renal impairment or dehydration. Magnesium sulfate can cause renal toxicity or fluid retention, which can affect the urinary output. The nurse should monitor the client's urinary output and fluid balance and report any abnormalities to the doctor.
D. Respiratory rate of 10 breaths/minute
Reason: This is incorrect because respiratory rate of 10 breaths/minute is below the normal range of 12 to 20 breaths/minute and may indicate respiratory depression. Magnesium sulfate can cause respiratory depression or failure, which can be life-threatening. The nurse should monitor the client's respiratory rate and oxygen saturation and administer oxygen or antidote if needed.
Full Explanation
Choice A Reason: This is incorrect because difficulty in arousing is a sign of magnesium toxicity, which is a serious complication of magnesium sulfate therapy. Magnesium toxicity can cause central nervous system depression, muscle weakness, and cardiac arrest. The nurse should monitor the client's level of consciousness and stop the infusion if the client becomes lethargic or unresponsive.
Choice B Reason: This is correct because deep tendon reflexes 2+ indicate a normal and expected response to magnesium sulfate therapy. Magnesium sulfate is a muscle relaxant that can reduce the risk of seizures in gestational hypertension. The nurse should assess the client's deep tendon reflexes regularly and maintain them at 2+ or slightly diminished.
Choice C Reason: This is incorrect because urinary output of 30 mL per hour is below the normal range of 40 to 80 mL per hour and may indicate renal impairment or dehydration. Magnesium sulfate can cause renal toxicity or fluid retention, which can affect the urinary output. The nurse should monitor the client's urinary output and fluid balance and report any abnormalities to the doctor.
Choice D Reason: This is incorrect because respiratory rate of 10 breaths/minute is below the normal range of 12 to 20 breaths/minute and may indicate respiratory depression. Magnesium sulfate can cause respiratory depression or failure, which can be life-threatening. The nurse should monitor the client's respiratory rate and oxygen saturation and administer oxygen or antidote if needed.