Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
The child is a 2-year-old who fell into a pool. He was retrieved from the pool by a family member but was not breathing. The family member started CPR, and the ambulance brought him to the hospital.
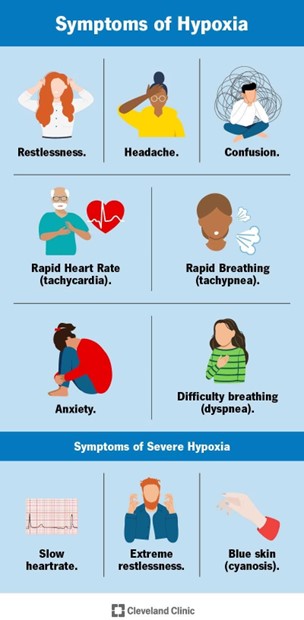
What factors are important in determining the level of hypoxemia that the child may have experienced during the submersion?
Select all that apply.
A. Temperature of water
Cold water can induce a diving reflex, which lowers the heart rate and oxygen consumption, and may protect the brain from hypoxic injury¹². Cold water can also cause laryngospasm, which prevents water aspiration but also impairs gas exchange
B. The weight of the child
This may affect the buoyancy and the ability to float or swim, but not the oxygen consumption or gas exchange during submersion¹.
C. Oxygen concentration of the ambient air
This may affect the pre-submersion oxygen saturation, but not the rate of oxygen depletion or gas exchange during submersion.
D. Whether or not anyone witnessed the fall into the pool
This may affect the time to rescue and resuscitation, but not the level of hypoxemia during submersion
E. The amount of time the child was submerged
The longer the submersion, the more severe the hypoxemia and the higher the risk of brain damage and death. The survival rate decreases significantly after 5 minutes of submersion
This question is an excerpt from Nurse Dive's nursing test bank - HESI PN Exit 2023 II Proctored Exam. Take the full exam now
Full Explanation
The level of hypoxemia that the child may have experienced during the submersion depends on several factors, but the most important ones are:
- The **temperature of water**: Cold water can induce a diving reflex, which lowers the heart rate and oxygen consumption, and may protect the brain from hypoxic injury. Cold water can also cause laryngospasm, which prevents water aspiration but also impairs gas exchange.
- The **amount of time the child was submerged**: The longer the submersion, the more severe the hypoxemia and the higher the risk of brain damage and death. The survival rate decreases significantly after 5 minutes of submersion.
The other factors are less relevant or not directly related to the level of hypoxemia:
- The **weight of the child**: This may affect the buoyancy and the ability to float or swim, but not the oxygen consumption or gas exchange during submersion.
- The **oxygen concentration of the ambient air**: This may affect the pre-submersion oxygen saturation, but not the rate of oxygen depletion or gas exchange during submersion.
- The **witnessing of the fall into the pool**: This may affect the time to rescue and resuscitation, but not the level of hypoxemia during submersion.
Similar Questions
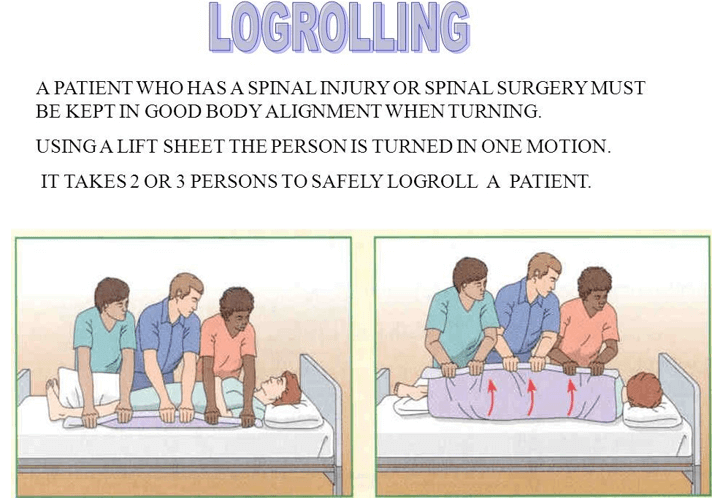
Immediately after log-rolling a client to a lateral position, which intervention should the practical nurse (PN) implement?
A. Raise the head of the bed 30 degrees
Raising the head of the bed 30 degrees is not necessary or appropriate after log-rolling a client to a lateral position, as it can cause shearing forces or compromise the spinal stability. The head of the bed should be kept flat or slightly elevated during log-rolling
B. Measure blood pressure and pulse rate
Measuring blood pressure and pulse rate is not the immediate intervention after log-rolling a client to a lateral position, as it does not ensure the comfort or safety of the client. The PN should monitor the vital signs before and after log-rolling, but not during or immediately after.
C. Flex legs and place blanket between legs
Flexing legs and placing blanket between legs is not the immediate intervention after log-rolling a client to a lateral position, as it does not support the spine or prevent pressure ulcers or nerve damage. The PN should keep the legs straight and aligned with the body during log-rolling, and place a pillow under the lower leg after log-rolling.
D. Place pillows to maintain alignment.
Log-rolling is a technique of moving a client as a unit without twisting or bending the spine, which is used for clients with spinal injuries or surgeries. After log-rolling a client to a lateral position, the PN should place pillows to maintain alignment and prevent pressure ulcers or nerve damage. The pillows should be placed under the head, neck, upper arm, chest, abdomen, pelvis, and lower leg.
Full Explanation
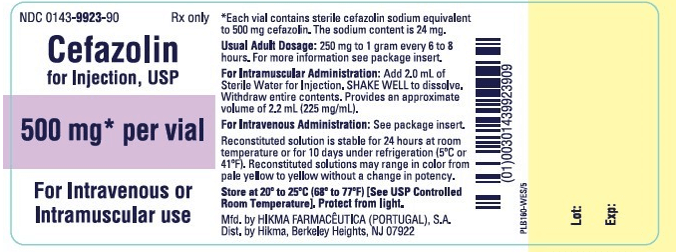
The practical nurse (PN) is preparing cefazolin 400 mg IM for a client with a gram-positive infection. The available vial is labeled, "Cefazolin 1 gram," and the instructions for reconstitution state, for IM use, add 2 mL sterile water for injection. Total volume after reconstitution is 2.5 mL. After reconstitution, how many mL should be administered to the client? (Enter numeric value only. If rounding is required, round to the whole number, nearest tenths/hundredth).
Full Explanation
This is the correct answer because the concentration of cefazolin after reconstitution is 1 gram/2.5 mL, which is equivalent to 400 mg/1 mL. Therefore, to administer 400 mg of cefazolin, the PN should draw up 1 mL of the reconstituted solution. This can be calculated using the formula:
Desired dose / Available dose = Volume to administer
400 mg / 1000 mg = x mL / 2.5 mL
x = (400 x 2.5) / 1000
x = 1 mL
The practical nurse (PN) believes that a prescription for a child is incorrect because the dosage prescribed is the usual adult dosage. Which action should the PN take?
A. Tell the pharmacy to send an accurate child's dosage
This is not the action that the PN should take if they believe that a prescription for a child is incorrect because the dosage prescribed is the usual adult dosage. Telling the pharmacy to send an accurate child's dosage is not appropriate, as it may cause confusion, delay, or conflict with the healthcare provider's orders. The PN should not assume that they know the correct dosage for the child without consulting with the healthcare provider.
B. Ask another nurse if adult dosages are ever given to children
This is not the action that the PN should take if they believe that a prescription for a child is incorrect because the dosage prescribed is the usual adult dosage. Asking another nurse if adult dosages are ever given to children is not helpful, as it may not provide accurate or reliable information. The PN should not rely on another nurse's opinion or experience without verifying it with the healthcare provider.
C. Call the healthcare provider and clarify the prescription
This is the action that the PN should take if they believe that a prescription for a child is incorrect because the dosage prescribed is the usual adult dosage. Calling the healthcare provider and clarifying the prescription is the safest and most effective way to prevent medication errors and ensure the child's safety. The PN should not administer the medication until they are sure that it is correct and appropriate for the child.
D. Request verification of the prescription by the charge nurse
This is not the action that the PN should take if they believe that a prescription for a child is incorrect because the dosage prescribed is the usual adult dosage. Requesting verification of the prescription by the charge nurse is not necessary, as it may waste time and resources. The PN should be able to communicate directly with the healthcare provider and clarify any doubts or concerns about the prescription.
Full Explanation
c) Call the healthcare provider and clarify the prescription. Correct
This is the action that the PN should take if they believe that a prescription for a child is incorrect because the dosage prescribed is the usual adult dosage.
Calling the healthcare provider and clarifying the prescription is the safest and most effective way to prevent medication errors and ensure the child's safety. The PN should not administer the medication until they are sure that it is correct and appropriate for the child.
a) Tell the pharmacy to send an accurate child's dosage.
This is not the action that the PN should take if they believe that a prescription for a child is incorrect because the dosage prescribed is the usual adult dosage.
Telling the pharmacy to send an accurate child's dosage is not appropriate, as it may cause confusion, delay, or conflict with the healthcare provider's orders. The PN should not assume that they know the correct dosage for the child without consulting with the healthcare provider.
b) Ask another nurse if adult dosages are ever given to children.
This is not the action that the PN should take if they believe that a prescription for a child is incorrect because the dosage prescribed is the usual adult dosage. Asking another nurse if adult dosages are ever given to children is not helpful, as it may not provide accurate or reliable information.
The PN should not rely on another nurse's opinion or experience without verifying it with the healthcare provider.
d) Request verification of the prescription by the charge nurse.
This is not the action that the PN should take if they believe that a prescription for a child is incorrect because the dosage prescribed is the usual adult dosage. Requesting verification of the prescription by the charge nurse is not necessary, as it may waste time and resources.
The PN should be able to communicate directly with the healthcare provider and clarify any doubts or concerns about the prescription.