Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
The client inquires what the positive result from the potassium hydroxide (KOH) test indicates. Which of the following is an accurate response by the nurse?
A. You have a virus.
Reason: A virus is not detected by the KOH test, which is used to diagnose fungal infections of the skin, hair, or nails. A virus can be detected by other tests, such as polymerase chain reaction (PCR) or viral culture.
B. You have a fungal infection.
Reason: A fungal infection is detected by the KOH test, which dissolves the skin cells and leaves behind the fungal elements that can be seen under a microscope. A fungal infection can cause symptoms such as itching, scaling, redness, or blisters.
C. You have a bacterial infection.
Reason: A bacterial infection is not detected by the KOH test, which is specific for fungi. A bacterial infection can be detected by other tests, such as gram stain or culture.
D. You have cancer.
Reason: Cancer is not detected by the KOH test, which is not a screening tool for malignancy. Cancer can be detected by other tests, such as biopsy or imaging.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Proctored Exam 4. Take the full exam now
Full Explanation
Choice A Reason: A virus is not detected by the KOH test, which is used to diagnose fungal infections of the skin, hair, or nails. A virus can be detected by other tests, such as polymerase chain reaction (PCR) or viral culture.
Choice B Reason: A fungal infection is detected by the KOH test, which dissolves the skin cells and leaves behind the fungal elements that can be seen under a microscope. A fungal infection can cause symptoms such as itching, scaling, redness, or blisters.
Choice C Reason: A bacterial infection is not detected by the KOH test, which is specific for fungi. A bacterial infection can be detected by other tests, such as gram stain or culture.
Choice D Reason: Cancer is not detected by the KOH test, which is not a screening tool for malignancy. Cancer can be detected by other tests, such as biopsy or imaging.
Similar Questions
A nurse in the emergency department is caring for a client who has extensive partial and full-thickness burns on the head, neck, and chest. The nurse should identify which of the following risks is the priority for assessment and intervention.
A. Airway obstruction.
reason: This is the correct answer because airway obstruction is the risk that is the priority for assessment and intervention for a client who has extensive partial and full-thickness burns of the head, neck, and chest. Airway obstruction can occur due to edema, inflammation, or inhalation injury of the upper airway structures. It can compromise oxygenation and ventilation, and lead to respiratory failure or cardiac arrest. The nurse should assess for signs of airway obstruction, such as stridor, hoarseness, dyspnea, or cyanosis, and provide oxygen therapy, humidification, or intubation as needed.
B. Fluid imbalance.
reason: This is incorrect because fluid imbalance is not the risk that is the priority for assessment and intervention for a client who has extensive partial and full-thickness burns of the head, neck, and chest. Fluid imbalance can occur due to fluid loss from damaged skin and capillaries, as well as increased capillary permeability and fluid shifts. It can cause dehydration, hypovolemia, shock, or electrolyte imbalances. The nurse should monitor fluid status, vital signs, urine output, and laboratory values, and provide fluid resuscitation as prescribed, but only after ensuring airway patency.
C. Paralytic ileus.
reason: This is incorrect because paralytic ileus is not the risk that is the priority for assessment and intervention for a client who has extensive partial and full-thickness burns of the head, neck, and chest. Paralytic ileus is a condition where there is decreased or absent bowel motility due to nerve damage or decreased blood flow to the gastrointestinal tract. It can cause abdominal distension, nausea, vomiting, or constipation. The nurse should assess bowel sounds, abdominal girth, and stool characteristics, and provide nasogastric suction or laxatives as prescribed, but only after ensuring airway patency and fluid balance.
D. Infection.
reason: This is incorrect because infection is not the risk that is the priority for assessment and intervention for a client who has extensive partial and full-thickness burns of the head, neck, and chest. Infection can occur due to loss of skin barrier, exposure to microorganisms, or impaired immune system. It can cause fever, increased pain, purulent drainage, or sepsis. The nurse should assess for signs of infection, obtain wound cultures, and administer antibiotics as prescribed, but only after ensuring airway patency, fluid balance, and pain control.
Full Explanation
Choice A reason: This is the correct answer because airway obstruction is the risk that is the priority for assessment and intervention for a client who has extensive partial and full-thickness burns of
the head, neck, and chest. Airway obstruction can occur due to edema, inflammation, or inhalation injury of
the upper airway structures. It can compromise oxygenation and ventilation, and lead to respiratory failure or cardiac arrest. The nurse should assess for signs of airway obstruction, such as stridor, hoarseness, dyspnea, or cyanosis, and provide oxygen therapy, humidification, or intubation as needed.
Choice B reason: This is incorrect because fluid imbalance is not the risk that is the priority for assessment and intervention for a client who has extensive partial and full-thickness burns of
the head, neck, and chest. Fluid imbalance can occur due to fluid loss from damaged skin and capillaries, as well as increased capillary permeability and fluid shifts. It can cause dehydration, hypovolemia, shock, or electrolyte imbalances. The nurse should monitor fluid status, vital signs, urine output, and laboratory values, and provide fluid resuscitation as prescribed, but only after ensuring airway patency.
Choice C reason: This is incorrect because paralytic ileus is not the risk that is the priority for assessment and intervention for a client who has extensive partial and full-thickness burns of
the head, neck, and chest. Paralytic ileus is a condition where there is decreased or absent bowel motility due to nerve damage or decreased blood flow to
the gastrointestinal tract. It can cause abdominal distension, nausea, vomiting, or constipation. The nurse should assess bowel sounds, abdominal girth, and stool characteristics, and provide nasogastric suction or laxatives as prescribed, but only after ensuring airway patency and fluid balance.
Choice D reason: This is incorrect because infection is not the risk that is the priority for assessment and intervention for a client who has extensive partial and full-thickness burns of
the head, neck, and chest. Infection can occur due to loss of skin barrier, exposure to microorganisms, or impaired immune system. It can cause fever, increased pain, purulent drainage, or sepsis. The nurse should assess for signs of infection, obtain wound cultures, and administer antibiotics as prescribed, but only after ensuring airway patency, fluid balance, and pain control.
A client arrives to the emergency department complaining of acute onset of nausea with projectile vomiting. The nurse's assessment findings include high-pitched sounds in the left upper quadrant. Which gastrointestinal disorder is consistent with these findings?
A. Colorectal cancer
Reason: Colorectal cancer is not likely to cause nausea with projectile vomiting or high-pitched sounds in the left upper quadrant. Colorectal cancer may cause symptoms such as rectal bleeding, change in bowel habits, abdominal pain, or weight loss.
B. Paralytic ileus
Reason: Paralytic ileus is a condition where the bowel stops working and does not contract or move food along. Paralytic ileus may cause symptoms such as abdominal distension, absence of bowel sounds, constipation, or vomiting.
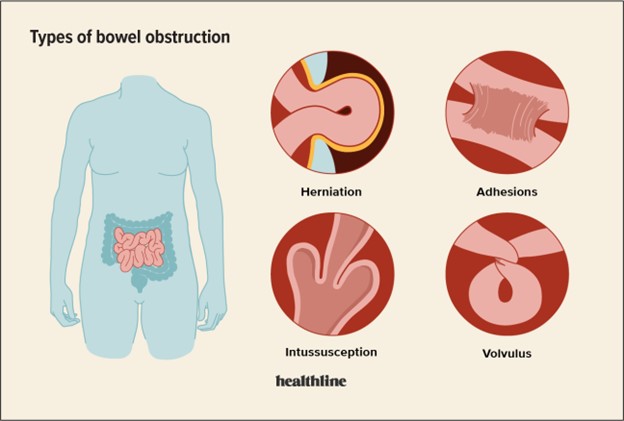
C. Large bowel obstruction
Reason: Large bowel obstruction is a blockage of the colon or rectum that prevents the passage of stool. Large bowel obstruction may cause symptoms such as abdominal distension, low-pitched sounds in the right lower quadrant, constipation, or ribbon-like stools.
D. Small bowel obstruction
Reason: Small bowel obstruction is a blockage of the small intestine that prevents the passage of food and fluids. Small bowel obstruction may cause symptoms such as nausea with projectile vomiting, high-pitched sounds in the left upper quadrant, abdominal cramps, or dehydration.
Full Explanation
Choice A Reason: Colorectal cancer is not likely to cause nausea with projectile vomiting or high-pitched sounds in the left upper quadrant. Colorectal cancer may cause symptoms such as rectal bleeding, change in bowel habits, abdominal pain, or weight loss.
Choice B Reason: Paralytic ileus is a condition where the bowel stops working and does not contract or move food along. Paralytic ileus may cause symptoms such as abdominal distension, absence of bowel sounds, constipation, or vomiting.
Choice C Reason: Large bowel obstruction is a blockage of the colon or rectum that prevents the passage of stool. Large bowel obstruction may cause symptoms such as abdominal distension, low-pitched sounds in the right lower quadrant, constipation, or ribbon-like stools.
Choice D Reason: Small bowel obstruction is a blockage of the small intestine that prevents the passage of food and fluids. Small bowel obstruction may cause symptoms such as nausea with projectile vomiting, high-pitched sounds in the left upper quadrant, abdominal cramps, or dehydration.
A nurse is teaching a class about physiological changes to hearing in older adult clients. Which of the following should the nurse include?
A. Decreased thickness of tympanic membranes
Reason: Decreased thickness of tympanic membranes is not a physiological change to hearing in older adult clients. The tympanic membranes are thin and flexible structures that vibrate in response to sound waves. The thickness of the tympanic membranes does not change significantly with age.
B. Decreased tinnitus
Reason: Decreased tinnitus is not a physiological change to hearing in older adult clients. Tinnitus is a ringing or buzzing sound in the ears that may be caused by various factors, such as noise exposure, ear infections, medications, or aging. Tinnitus may increase or decrease with age, depending on the underlying cause.
C. Decreased ear wax
Reason: Decreased ear wax is not a physiological change to hearing in older adult clients. Ear wax is a natural substance that lubricates and protects the ear canal from dust, bacteria, and insects. Ear wax production may vary with age, but it does not affect hearing unless it accumulates and blocks the ear canal.
D. Decreased ability to hear high-frequency sounds
Reason: Decreased ability to hear high-frequency sounds is a physiological change to hearing in older adult clients. This is also known as presbycusis, which is a gradual loss of hearing that occurs as part of aging. Presbycusis affects the ability to hear high-pitched sounds, such as consonants, birdsong, or alarms.
Full Explanation
Choice A Reason: Decreased thickness of tympanic membranes is not a physiological change to hearing in older adult clients. The tympanic membranes are thin and flexible structures that vibrate in response to sound waves. The thickness of the tympanic membranes does not change significantly with age.
Choice B Reason: Decreased tinnitus is not a physiological change to hearing in older adult clients. Tinnitus is a ringing or buzzing sound in the ears that may be caused by various factors, such as noise exposure, ear infections, medications, or aging. Tinnitus may increase or decrease with age, depending on the underlying cause.
Choice C Reason: Decreased ear wax is not a physiological change to hearing in older adult clients. Ear wax is a natural substance that lubricates and protects the ear canal from dust, bacteria, and insects. Ear wax production may vary with age, but it does not affect hearing unless it accumulates and blocks the ear canal.
Choice D Reason: Decreased ability to hear high-frequency sounds is a physiological change to hearing in older adult clients. This is also known as presbycusis, which is a gradual loss of hearing that occurs as part of aging. Presbycusis affects the ability to hear high-pitched sounds, such as consonants, birdsong, or alarms.