Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
The doctor orders dextrose 5% in water 1,000 mL to be infused over 8 hours. The IV tubing delivers 15 drops per milliliter. The nurse in charge should run the IV infusion at a rate of:
NOTE: Enter ONLY THE NUMBER DO NOT enter the unit of measurement
This question is an excerpt from Nurse Dive's nursing test bank - Final Med Surg Comprehensive Proctored Exam (Brooklyn University). Take the full exam now
Full Explanation
Let’s calculate the IV infusion rate step by step.
Step 1: Determine the total volume to be infused.
The total volume ordered is 1,000 mL.
Step 2: Determine the total time for the infusion.
The total time is 8 hours.
Step 3: Calculate the infusion rate in mL per hour.
Total volume (1,000 mL) ÷ Total time (8 hours) = 125 mL per hour.
Result: 125
Step 4: Determine the drop factor.
The IV tubing delivers 15 drops per milliliter.
Step 5: Calculate the infusion rate in drops per minute.
Infusion rate (125 mL per hour) × Drop factor (15 drops per mL) = 1,875 drops per hour.
Result: 1,875
Step 6: Convert the infusion rate to drops per minute.
Total drops per hour (1,875 drops) ÷ 60 minutes = 31.25 drops per minute.
Result: 31.25
Step 7: Round the result to the nearest whole number if necessary.
31.25 rounded to the nearest whole number is 31.
The nurse should run the IV infusion at a rate of 31 drops per minute.
Similar Questions
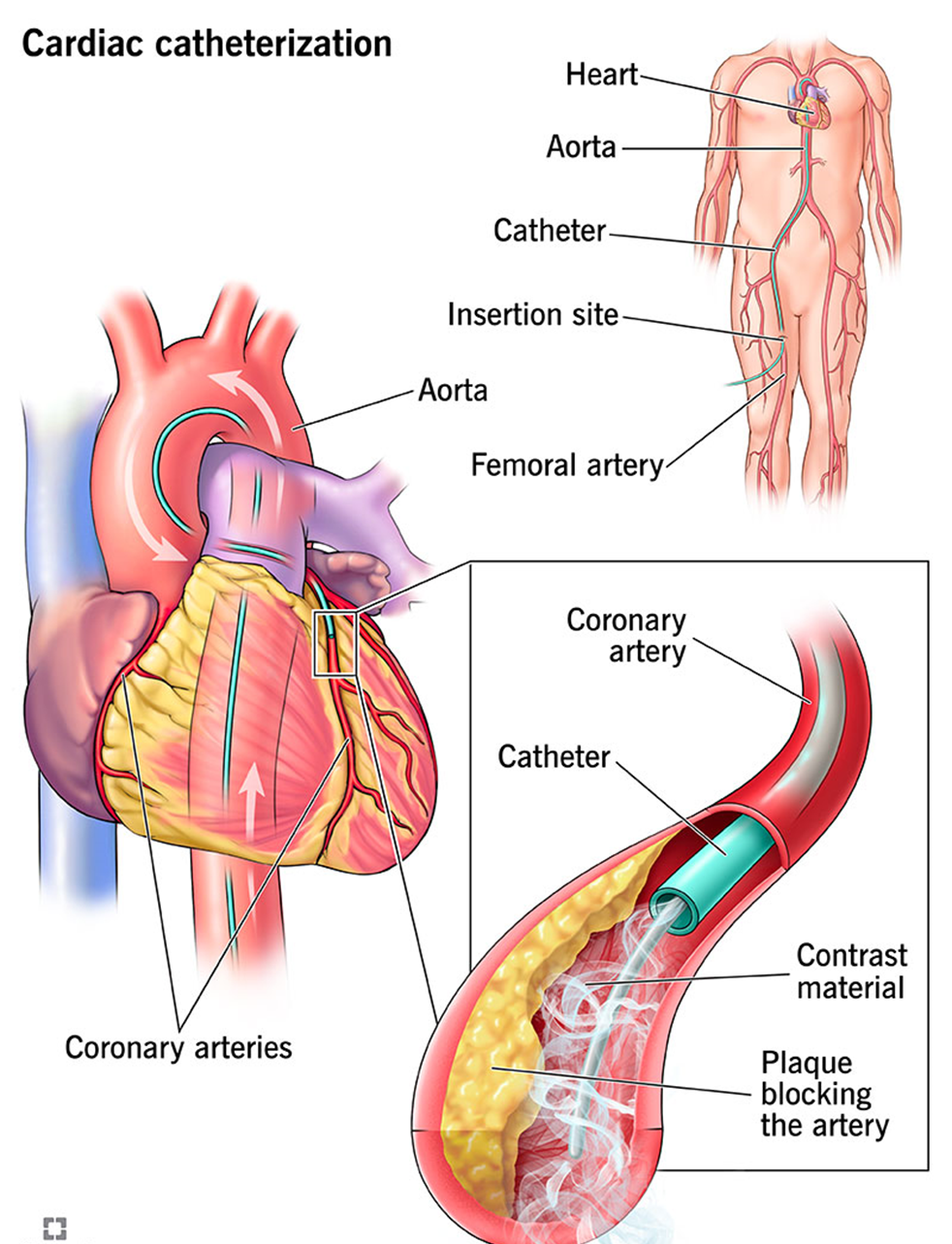
A nurse is collecting a medication history from a client who is scheduled to have a cardiac catheterization. Which of the following medications taken by the client interacts with contrast material and places the client at risk for acute kidney injury?
A. Metformin
Metformin is known to interact with contrast material, particularly iodinated contrast media, and can increase the risk of acute kidney injury (AKI). This interaction can lead to a condition known as contrast-induced nephropathy (CIN) or contrast-induced acute kidney injury (CI-AKI). Metformin is primarily excreted by the kidneys, and impaired renal function can lead to its accumulation, increasing the risk of lactic acidosis, a rare but serious complication. Therefore, it is generally recommended to withhold metformin before and after the administration of contrast media until renal function is confirmed to be normal.
B. Carvedilol
Carvedilol is a beta-blocker used to treat high blood pressure and heart failure. It does not have a known interaction with contrast media that would increase the risk of acute kidney injury. Carvedilol primarily affects the cardiovascular system and does not significantly impact renal function or interact with contrast agents.
C. Nitroglycerin
Nitroglycerin is used to treat angina and other heart conditions by dilating blood vessels. It does not interact with contrast media in a way that would increase the risk of acute kidney injury. Nitroglycerin’s primary effects are on the cardiovascular system, and it does not have nephrotoxic properties.
D. Atorvastatin
Atorvastatin is a statin used to lower cholesterol levels. While it can have effects on liver enzymes and muscle tissue, it does not interact with contrast media to increase the risk of acute kidney injury. Atorvastatin is metabolized by the liver and does not significantly impact renal function.
E. None
None
F. None
None
Full Explanation
Choice A: Metformin
Reason: Metformin is known to interact with contrast material, particularly iodinated contrast media, and can increase the risk of acute kidney injury (AKI). This interaction can lead to a condition known as contrast-induced nephropathy (CIN) or contrast-induced acute kidney injury (CI-AKI). Metformin is primarily excreted by the kidneys, and impaired renal function can lead to its accumulation, increasing the risk of lactic acidosis, a rare but serious complication. Therefore, it is generally recommended to withhold metformin before and after the administration of contrast media until renal function is confirmed to be normal.
Choice B: Carvedilol
Reason: Carvedilol is a beta-blocker used to treat high blood pressure and heart failure. It does not have a known interaction with contrast media that would increase the risk of acute kidney injury. Carvedilol primarily affects the cardiovascular system and does not significantly impact renal function or interact with contrast agents.
Choice C: Nitroglycerin
Reason: Nitroglycerin is used to treat angina and other heart conditions by dilating blood vessels. It does not interact with contrast media in a way that would increase the risk of acute kidney injury. Nitroglycerin’s primary effects are on the cardiovascular system, and it does not have nephrotoxic properties.
Choice D: Atorvastatin
Reason: Atorvastatin is a statin used to lower cholesterol levels. While it can have effects on liver enzymes and muscle tissue, it does not interact with contrast media to increase the risk of acute kidney injury. Atorvastatin is metabolized by the liver and does not significantly impact renal function.
A nurse is caring for a client who is scheduled to undergo a thoracentesis. Which intervention would the nurse complete prior to the procedure? The nurse assesses the client after a thoracentesis. Which assessment finding warrants immediate action? You should have 2 responses for this question: 1 for Intervention and 1 for Assessment.
A. Assessment: The trachea is shifted away from the midline of the neck.
Reason: A tracheal shift is a critical finding that warrants immediate action. It can indicate a tension pneumothorax, which is a life-threatening condition where air accumulates in the pleural space and causes the lung to collapse. This shift can compromise respiratory function and requires urgent intervention34.
B. Assessment: Pulse oximetry is 93% on 2 L of oxygen.
Reason: While a pulse oximetry reading of 93% on 2 liters of oxygen is slightly below the normal range (95-100%), it is not immediately life-threatening. However, it does indicate that the client may need further evaluation and monitoring to ensure adequate oxygenation.
C. Assessment: The client rates pain as 8/10 at the site of the procedure.
Reason: Pain management is important, but an 8/10 pain rating at the procedure site, while significant, does not require immediate action compared to a tracheal shift. Pain can be managed with appropriate analgesics as ordered by the physician.
D. Intervention: Request an order for pain medication.
Requesting an order for pain medication is a necessary intervention for managing the client’s pain, but it is not as urgent as addressing a tracheal shift. Pain management should be part of the overall care plan.
E. Intervention: Measure oxygen saturation before and after a 12-minute walk.
Reason: Measuring oxygen saturation before and after a 12-minute walk is a useful assessment to evaluate the client’s respiratory function and endurance. However, it is not an immediate priority compared to ensuring informed consent and addressing critical findings.
F. Intervention: Explain the procedure in detail to the client and the family.
Reason: Explaining the procedure in detail to the client and their family is essential for informed consent and reducing anxiety. It ensures that the client understands what to expect and can make an informed decision about their care.
G. Intervention: Assist the client to the bathroom.
Reason: Assisting the client to the bathroom is a routine nursing intervention that ensures the client’s comfort and dignity. However, it is not a priority compared to addressing critical findings and ensuring informed consent.
H. Intervention: Discuss all possible complications with the client.
Reason: Discussing all possible complications with the client is part of the informed consent process. It ensures that the client is aware of potential risks and can make an informed decision about their care.
I. Assessment: A small amount of drainage from the site is noted.
Reason: Noting a small amount of drainage from the site is an important assessment, but it is not as urgent as addressing a tracheal shift. The drainage should be monitored and documented, and any significant changes should be reported to the physician.
J. Intervention: Validate that informed consent has been given by the client.
Reason: Before any invasive procedure, it is crucial to ensure that the client has given informed consent. This means the client understands the procedure, its risks, benefits, and any potential complications. Validating informed consent is a legal and ethical requirement that ensures the client is making an informed decision about their care12.
Full Explanation
Intervention: Validate that informed consent has been given by the client.
Reason: Before any invasive procedure, it is crucial to ensure that the client has given informed consent. This means the client understands the procedure, its risks, benefits, and any potential complications. Validating informed consent is a legal and ethical requirement that ensures the client is making an informed decision about their care12.
Assessment: The trachea is shifted away from the midline of the neck.
Reason: A tracheal shift is a critical finding that warrants immediate action. It can indicate a tension pneumothorax, which is a life-threatening condition where air accumulates in the pleural space and causes the lung to collapse. This shift can compromise respiratory function and requires urgent intervention34.
Choice B: Pulse oximetry is 93% on 2 L of oxygen.
Reason: While a pulse oximetry reading of 93% on 2 liters of oxygen is slightly below the normal range (95-100%), it is not immediately life-threatening. However, it does indicate that the client may need further evaluation and monitoring to ensure adequate oxygenation.
Choice C: The client rates pain as 8/10 at the site of the procedure.
Reason: Pain management is important, but an 8/10 pain rating at the procedure site, while significant, does not require immediate action compared to a tracheal shift. Pain can be managed with appropriate analgesics as ordered by the physician.
Choice D: Request an order for pain medication.
Reason: Requesting an order for pain medication is a necessary intervention for managing the client’s pain, but it is not as urgent as addressing a tracheal shift. Pain management should be part of the overall care plan.
Choice E: Measure oxygen saturation before and after a 12-minute walk.
Reason: Measuring oxygen saturation before and after a 12-minute walk is a useful assessment to evaluate the client’s respiratory function and endurance. However, it is not an immediate priority compared to ensuring informed consent and addressing critical findings.
Choice F: Explain the procedure in detail to the client and the family.
Reason: Explaining the procedure in detail to the client and their family is essential for informed consent and reducing anxiety. It ensures that the client understands what to expect and can make an informed decision about their care.
Choice G: Assist the client to the bathroom.
Reason: Assisting the client to the bathroom is a routine nursing intervention that ensures the client’s comfort and dignity. However, it is not a priority compared to addressing critical findings and ensuring informed consent.
Choice H: Discuss all possible complications with the client.
Reason: Discussing all possible complications with the client is part of the informed consent process. It ensures that the client is aware of potential risks and can make an informed decision about their care.
Choice I: A small amount of drainage from the site is noted.
Reason: Noting a small amount of drainage from the site is an important assessment, but it is not as urgent as addressing a tracheal shift. The drainage should be monitored and documented, and any significant changes should be reported to the physician.
After teaching a nursing student about mitral valve stenosis and mitral valve regurgitation, the nurse identifies effective learning when the student identifies which common feature of both disorders?
A. Hemoptysis
: Hemoptysis, or coughing up blood, is a common feature of both mitral valve stenosis and mitral valve regurgitation. In mitral valve stenosis, the narrowing of the valve leads to increased pressure in the pulmonary veins, which can cause pulmonary congestion and hemoptysis. Similarly, in mitral valve regurgitation, the backflow of blood into the left atrium increases pulmonary pressure, potentially leading to pulmonary edema and hemoptysis. Therefore, hemoptysis is a shared symptom of both conditions.
B. High-pitched holosystolic murmur
: A high-pitched holosystolic murmur is more commonly associated with mitral valve regurgitation rather than mitral valve stenosis. In mitral valve regurgitation, the murmur is caused by the backflow of blood from the left ventricle into the left atrium during systole3. Mitral valve stenosis, on the other hand, typically presents with a diastolic murmur due to the turbulent flow of blood through the narrowed valve during diastole. Therefore, a high-pitched holosystolic murmur is not a common feature of both disorders.
C. Hepatomegaly
: Hepatomegaly, or an enlarged liver, can occur in advanced cases of both mitral valve stenosis and mitral valve regurgitation due to right-sided heart failure. However, it is not a primary or common feature of these conditions. Hepatomegaly is more often associated with conditions that directly affect the right side of the heart or cause systemic congestion. Therefore, hepatomegaly is not a common feature of both mitral valve stenosis and mitral valve regurgitation.
Full Explanation
Choice A Reason:
Hemoptysis, or coughing up blood, is a common feature of both mitral valve stenosis and mitral valve regurgitation. In mitral valve stenosis, the narrowing of the valve leads to increased pressure in the pulmonary veins, which can cause pulmonary congestion and hemoptysis. Similarly, in mitral valve regurgitation, the backflow of blood into the left atrium increases pulmonary pressure, potentially leading to pulmonary edema and hemoptysis. Therefore, hemoptysis is a shared symptom of both conditions.
Choice B Reason:
A high-pitched holosystolic murmur is more commonly associated with mitral valve regurgitation rather than mitral valve stenosis. In mitral valve regurgitation, the murmur is caused by the backflow of blood from the left ventricle into the left atrium during systole3. Mitral valve stenosis, on the other hand, typically presents with a diastolic murmur due to the turbulent flow of blood through the narrowed valve during diastole. Therefore, a high-pitched holosystolic murmur is not a common feature of both disorders.
Choice C Reason:
Hepatomegaly, or an enlarged liver, can occur in advanced cases of both mitral valve stenosis and mitral valve regurgitation due to right-sided heart failure. However, it is not a primary or common feature of these conditions. Hepatomegaly is more often associated with conditions that directly affect the right side of the heart or cause systemic congestion. Therefore, hepatomegaly is not a common feature of both mitral valve stenosis and mitral valve regurgitation.