Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A. Obtain postoperative vital signs for a client one day following unilateral knee arthroplasty.
B. Perform daily surgical dressing change for a client who had an abdominal hysterectomy.
C. Initiate patient controlled analgesia (PCA. pumps for two clients immediately postoperatively.
Initiating patient controlled analgesia (PCA. pumps for two clients immediately postoperatively is not a nursing action that can be assigned to the PN. PCA pump is a device that allows the client to self-administer pain medication through an IV line by pressing a button. PCA pump should be initiated by the nurse after verifying the prescription, setting the parameters, educating the client, and ensuring safety and effectiveness. The PN does not have the authority or competency to initiate PCA pump or adjust its settings.
D. Start the second blood transfusion for a client twelve hours following a below knee amputation.
Starting the second blood transfusion for a client twelve hours following a below knee amputation is not a nursing action that can be assigned to the PN. Blood transfusion is a procedure that delivers donated blood or blood products into the client's bloodstream through an IV line. Blood transfusion should be started by the nurse after verifying the prescription, checking the blood type and compatibility, obtaining informed consent, and monitoring for any adverse reactions. The PN does not have the authority or competency to start blood transfusion or manage its complications.
E. Monitor a dose of warfarin per protocol for a client with type 2 diabetes mellitus (DM).
This question is an excerpt from Nurse Dive's nursing test bank - HESI Exit II Proctored Exam. Take the full exam now
Full Explanation
Choice C reason: Initiating patient controlled analgesia (PCA. pumps for two clients immediately postoperatively is not a nursing action that can be assigned to the PN. PCA pump is a device that allows the client to self-administer pain medication through an IV line by pressing a button. PCA pump should be initiated by the nurse after verifying the prescription, setting the parameters, educating the client, and ensuring safety and effectiveness. The PN does not have the authority or competency to initiate PCA pump or adjust its settings.
Choice D reason: Starting the second blood transfusion for a client twelve hours following a below knee amputation is not a nursing action that can be assigned to the PN. Blood transfusion is a procedure that delivers donated blood or blood products into the client's bloodstream through an IV line. Blood transfusion should be started by the nurse after verifying the prescription, checking the blood type and compatibility, obtaining informed consent, and monitoring for any adverse reactions. The PN does not have the authority or competency to start blood transfusion or manage its complications.
Similar Questions
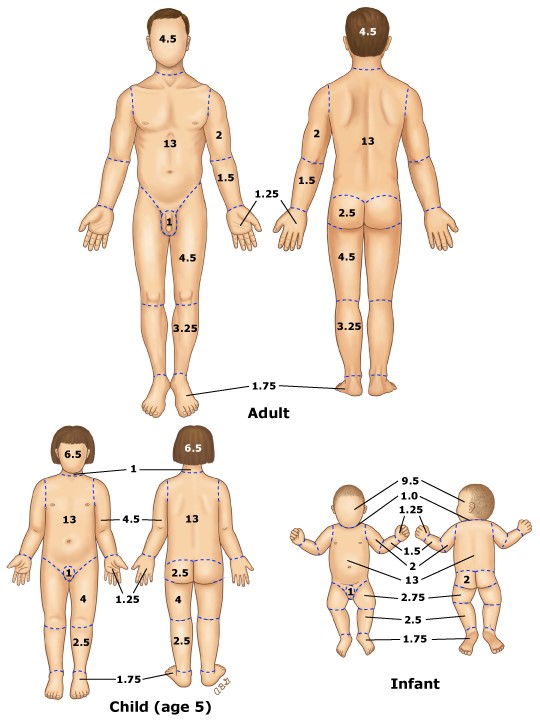
A patient experiences a gasoline tank fire when riding a motorcycle and is admitted to the emergency department (ED. with partial-thickness burns on the anterior surfaces of both lower extremities. Which percentage of body surface area should the nurse document in the electronic medical record (EMR)?
A. 18%.
This is the correct answer.According to the rule of nines, each leg accounts for 18% of the total body surface area, and the anterior surface of each leg accounts for half of that, or 9%. Therefore, the patient has partial-thickness burns on 9% + 9% = 18% of the body surface area.
B. 45%.
This is incorrect. This would be the case if the patient had partial-thickness burns on the anterior and posterior surfaces of both legs, as well as the head and neck, which is not given in the question.
C. 9%.
This is incorrect. This would be the case if the patient had partial-thickness burns on the anterior surface of only one leg, which is not given in the question.
D. 36%.
This is incorrect. This would be the case if the patient had partial-thickness burns on the anterior and posterior surfaces of both legs, which is not given in the question.
Full Explanation
Choice A reason: This is the correct answer. According to the rule of nines, each leg accounts for 18% of the total body surface area, and the anterior surface of each leg accounts for half of that, or 9%. Therefore, the patient has partial-thickness burns on 9% + 9% = 18% of the body surface area.
Choice B reason: This is incorrect. This would be the case if the patient had partial-thickness burns on the anterior and posterior surfaces of both legs, as well as the head and neck, which is not given in the question.
Choice C reason: This is incorrect. This would be the case if the patient had partial-thickness burns on the anterior surface of only one leg, which is not given in the question.
Choice D reason: This is incorrect. This would be the case if the patient had partial-thickness burns on the anterior and posterior surfaces of both legs, which is not given in the question.
The nurse is planning to teach infant care and preventive measures for sudden infant death syndrome (SIDS) to a group of new parents. Which information is most important for the nurse to include?
A. Ensure that the infant's crib mattress is firm.
This is correct because a firm mattress reduces the risk of suffocation and rebreathing of carbon dioxide, which are associated with SIDS.
B. Prop the infant with a pillow when in a side-lying position.
This is incorrect because propping the infant with a pillow can cause the infant to slide down and suffocate or obstruct the airway.
C. Swaddle the infant in a blanket for sleeping.
This is incorrect because swaddling the infant in a blanket can cause overheating, which is a risk factor for SIDS.
D. Place the infant in a prone position whenever possible.
This is incorrect because placing the infant in a prone position can increase the risk of SIDS by impairing gas exchange and thermoregulation.
Full Explanation
Choice A reason: This is correct because a firm mattress reduces the risk of suffocation and rebreathing of carbon dioxide, which are associated with SIDS.
Choice B reason: This is incorrect because propping the infant with a pillow can cause the infant to slide down and suffocate or obstruct the airway.
Choice C reason: This is incorrect because swaddling the infant in a blanket can cause overheating, which is a risk factor for SIDS.
Choice D reason: This is incorrect because placing the infant in a prone position can increase the risk of SIDS by impairing gas exchange and thermoregulation.
The nurse on a pediatric unit observes a distraught mother in the hallway scolding her 3-year-old son for wetting his pants. What initial action should the nurse take?
A. Provide disposable training pants while calming the mother.
This is correct because it addresses both the physical and emotional needs of the child and the mother. The nurse should provide comfort and reassurance to the mother and explain that occasional accidents are normal and not a sign of failure.
B. Refer the mother to a community parent education program.
This is incorrect because it implies that the mother is incompetent and needs external help. The nurse should first establish rapport and trust with the mother before suggesting any resources or interventions.
C. Suggest that the mother consult a pediatric nephrologist.
This is incorrect because it suggests that there is something wrong with the child's kidneys, which may alarm and offend the mother. The nurse should not jump to conclusions without assessing the child's history and symptoms.
D. Inform the mother that toilet training is slower for boys.
This is incorrect because it generalizes and stereotypes boys as being slower than girls in toilet training. The nurse should not make assumptions based on gender and should respect individual differences.
Full Explanation
Choice A reason: This is correct because it addresses both the physical and emotional needs of the child and the mother. The nurse should provide comfort and reassurance to the mother and explain that occasional accidents are normal and not a sign of failure.
Choice B reason: This is incorrect because it implies that the mother is incompetent and needs external help. The nurse should first establish rapport and trust with the mother before suggesting any resources or interventions.
Choice C reason: This is incorrect because it suggests that there is something wrong with the child's kidneys, which may alarm and offend the mother. The nurse should not jump to conclusions without assessing the child's history and symptoms.
Choice D reason: This is incorrect because it generalizes and stereotypes boys as being slower than girls in toilet training. The nurse should not make assumptions based on gender and should respect individual differences.