Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
The nurse provides instructions to a client diagnosed with inflammatory bowel syndrome (IBS) about measures to treat diarrhea caused by acute flare-ups. Which statement by the client indicates a need for further teaching?
A. "I will eat frequent small meals."
Reason: This is correct because eating frequent small meals can help the client with IBS to avoid overloading the digestive system and triggering diarrhea. The nurse should advise the client to eat slowly and chew well, and avoid foods that are spicy, fatty, or gas-producing.
B. "I will increase the intake of leafy greens and other sources of dietary fiber."
Reason: This is incorrect because increasing the intake of leafy greens and other sources of dietary fiber can worsen diarrhea by increasing stool bulk and motility. The nurse should advise the client to limit or avoid high-fiber foods, such as whole grains, fruits, vegetables, nuts, and seeds, during acute flare-ups of IBS. The client can gradually reintroduce fiber when the symptoms subside.
C. "I will increase fluids."
Reason: This is correct because increasing fluids can help the client with IBS to prevent dehydration and electrolyte imbalance caused by diarrhea. The nurse should advise the client to drink at least 8 glasses of water per day and avoid caffeinated, alcoholic, or carbonated beverages that can irritate the bowel or cause gas.
D. "I will take prescribed medications on schedule to regulate bowel patterns."
Reason: This is correct because taking prescribed medications on schedule can help the client with IBS to regulate bowel patterns and reduce diarrhea. The nurse should instruct the client on how to use medications, such as antidiarrheals, antispasmodics, or probiotics, as ordered by the provider. The nurse should also monitor the client for any adverse effects or interactions of the medications.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Proctored Exam 4. Take the full exam now
Full Explanation
Choice A Reason: This is correct because eating frequent small meals can help the client with IBS to avoid overloading the digestive system and triggering diarrhea. The nurse should advise the client to eat slowly and chew well, and avoid foods that are spicy, fatty, or gas-producing.
Choice B Reason: This is incorrect because increasing the intake of leafy greens and other sources of dietary fiber can worsen diarrhea by increasing stool bulk and motility. The nurse should advise the client to limit or avoid high-fiber foods, such as whole grains, fruits, vegetables, nuts, and seeds, during acute flare-ups of IBS. The client can gradually reintroduce fiber when the symptoms subside.
Choice C Reason: This is correct because increasing fluids can help the client with IBS to prevent dehydration and electrolyte imbalance caused by diarrhea. The nurse should advise the client to drink at least 8 glasses of water per day and avoid caffeinated, alcoholic, or carbonated beverages that can irritate the bowel or cause gas.
Choice D Reason: This is correct because taking prescribed medications on schedule can help the client with IBS to regulate bowel patterns and reduce diarrhea. The nurse should instruct the client on how to use medications, such as antidiarrheals, antispasmodics, or probiotics, as ordered by the provider. The nurse should also monitor the client for any adverse effects or interactions of the medications.
Similar Questions
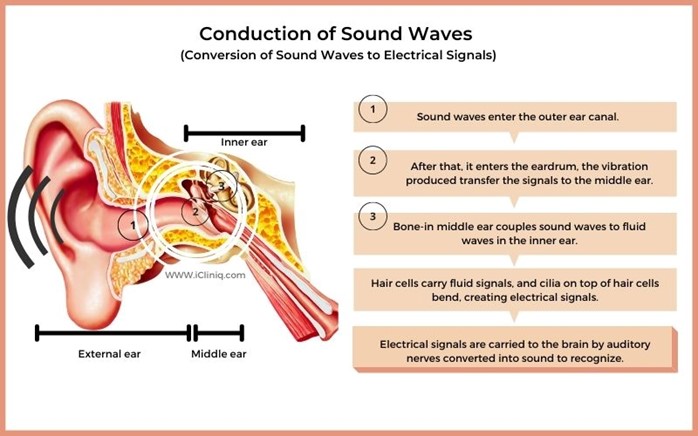
A nurse is caring for a client who has progressive presbycusis. Which of the following actions should the nurse take?
A. Use sign language when communicating with the client.
reason: This is incorrect because using sign language when communicating with the client is not an appropriate action for the nurse to take. Sign language is a form of communication that uses hand gestures, facial expressions, and body movements. It is not a universal language and requires training and practice. The nurse should not assume that the client knows or prefers sign language, unless they have indicated so.
B. Speak loudly and into the client's good ear.
reason: This is incorrect because speaking loudly and into the client's good ear is not an appropriate action for the nurse to take. Speaking loudly can distort the sound quality and cause discomfort or irritation to the client. Speaking into the client's good ear can also create a sense of imbalance and isolation. The nurse should speak at a normal volume and tone, and face the client directly.
C. Speak directly to the client in a normal, clear voice.
reason: This is the correct answer because speaking directly to the client in a normal, clear voice is an appropriate action for the nurse to take. Speaking directly to the client can help them see the nurse's mouth movements and facial expressions, which can enhance understanding and communication. Speaking in a normal, clear voice can help convey the message clearly and respectfully.
D. Sit by the client's side and speak very slowly.
reason: This is incorrect because sitting by the client's side and speaking very slowly is not an appropriate action for the nurse to take. Sitting by the client's side can make it difficult for them to see the nurse's face and hear their voice. Speaking very slowly can also make the message unclear and patronizing. The nurse should sit in front of the client and speak at a normal pace.
Full Explanation
Choice A reason: This is incorrect because using sign language when communicating with the client is not an appropriate action for the nurse to take. Sign language is a form of communication that uses hand gestures, facial expressions, and body movements. It is not a universal language and requires training and practice. The nurse should not assume that the client knows or prefers sign language unless they have indicated so.
Choice B reason: This is incorrect because speaking loudly and into the client's good ear is not an appropriate action for the nurse to take. Speaking loudly can distort the sound quality and cause discomfort or irritation to the client. Speaking into the client's good ear can also create a sense of imbalance and isolation. The nurse should speak at a normal volume and tone, and face the client directly.
Choice C reason: This is the correct answer because speaking directly to the client in a normal, clear voice is an appropriate action for the nurse to take. Speaking directly to the client can help them see the nurse's mouth movements and facial expressions, which can enhance understanding and communication. Speaking in a normal, clear voice can help convey the message clearly and respectfully.
Choice D reason: This is incorrect because sitting by the client's side and speaking very slowly is not an appropriate action for the nurse to take. Sitting by the client's side can make it difficult for them to see the nurse's face and hear their voice. Speaking very slowly can also make the message unclear and patronizing. The nurse should sit in front of the client and speak at a normal pace.
A nurse is caring for a client who has progressive presbycusis. Which of the following actions should the nurse take?
A. Use sign language when communicating with the client.
reason: This is incorrect because using sign language when communicating with the client is not an appropriate action for the nurse to take. Sign language is a form of communication that uses hand gestures, facial expressions, and body movements. It is not a universal language and requires training and practice. The nurse should not assume that the client knows or prefers sign language unless they have indicated so.
B. Speak loudly and into the client's good ear.
reason: This is incorrect because speaking loudly and into the client's good ear is not an appropriate action for the nurse to take. Speaking loudly can distort the sound quality and cause discomfort or irritation to the client. Speaking into the client's good ear can also create a sense of imbalance and isolation. The nurse should speak at a normal volume and tone, and face the client directly.
C. Speak directly to the client in a normal, clear voice.
reason: This is the correct answer because speaking directly to the client in a normal, clear voice is an appropriate action for the nurse to take. Speaking directly to the client can help them see the nurse's mouth movements and facial expressions, which can enhance understanding and communication. Speaking in a normal, clear voice can help convey the message clearly and respectfully.
D. Sit by the client's side and speak very slowly.
reason: This is incorrect because sitting by the client's side and speaking very slowly is not an appropriate action for the nurse to take. Sitting by the client's side can make it difficult for them to see the nurse's face and hear their voice. Speaking very slowly can also make the message unclear and patronizing. The nurse should sit in front of the client and speak at a normal pace.
Full Explanation
Choice A reason: This is incorrect because using sign language when communicating with the client is not an appropriate action for the nurse to take. Sign language is a form of communication that uses hand gestures, facial expressions, and body movements. It is not a universal language and requires training and practice. The nurse should not assume that the client knows or prefers sign language unless they have indicated so.
Choice B reason: This is incorrect because speaking loudly and into the client's good ear is not an appropriate action for the nurse to take. Speaking loudly can distort the sound quality and cause discomfort or irritation to the client. Speaking into the client's good ear can also create a sense of imbalance and isolation. The nurse should speak at a normal volume and tone, and face the client directly.
Choice C reason: This is the correct answer because speaking directly to the client in a normal, clear voice is an appropriate action for the nurse to take. Speaking directly to the client can help them see the nurse's mouth movements and facial expressions, which can enhance understanding and communication. Speaking in a normal, clear voice can help convey the message clearly and respectfully.
Choice D reason: This is incorrect because sitting by the client's side and speaking very slowly is not an appropriate action for the nurse to take. Sitting by the client's side can make it difficult for them to see the nurse's face and hear their voice. Speaking very slowly can also make the message unclear and patronizing. The nurse should sit in front of the client and speak at a normal pace.
A nurse is assessing a client who has suffered a traumatic brain injury. When the nurse applies a stimuli to the client, which of the following responses by the client indicates that the client has suffered an extensive cervical spine injury?
A. Nystagmus
Reason: This is incorrect because nystagmus is not a response to stimuli, but a condition that causes involuntary eye movements. Nystagmus can be caused by various factors, such as inner ear disorders, brain lesions, or drug toxicity, but not necessarily by cervical spine injury.
B. Decorticate positioning
Reason: This is incorrect because decorticate positioning is a response to stimuli that indicates damage to the cerebral cortex or the corticospinal tract. Decorticate positioning is characterized by flexion of the arms and extension of the legs. It does not indicate cervical spine injury, which affects the spinal cord below the brainstem.
C. Lack of any response
Reason: This is incorrect because lack of any response to stimuli can indicate various levels of brain damage or coma, but not specifically cervical spine injury. Lack of any response can also be influenced by other factors, such as sedation, hypothermia, or shock.
D. Decerebrate positioning
Reason: This is correct because decerebrate positioning is a response to stimuli that indicates damage to the brainstem or the upper cervical spine. Decerebrate positioning is characterized by extension and outward rotation of the arms and legs. It indicates a severe and life-threatening injury that can impair vital functions, such as breathing and blood pressure.
Full Explanation
Choice A Reason: This is incorrect because nystagmus is not a response to stimuli, but a condition that causes involuntary eye movements. Nystagmus can be caused by various factors, such as inner ear disorders, brain lesions, or drug toxicity, but not necessarily by cervical spine injury.
Choice B Reason: This is incorrect because decorticate positioning is a response to stimuli that indicates damage to the cerebral cortex or the corticospinal tract. Decorticate positioning is characterized by flexion of the arms and extension of the legs. It does not indicate cervical spine injury, which affects the spinal cord below the brainstem.
Choice C Reason: This is incorrect because lack of any response to stimuli can indicate various levels of brain damage or coma, but not specifically cervical spine injury. Lack of any response can also be influenced by other factors, such as sedation, hypothermia, or shock.
Choice D Reason: This is correct because decerebrate positioning is a response to stimuli that indicates damage to the brainstem or the upper cervical spine. Decerebrate positioning is characterized by extension and outward rotation of the arms and legs. It indicates a severe and life-threatening injury that can impair vital functions, such as breathing and blood pressure.