Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
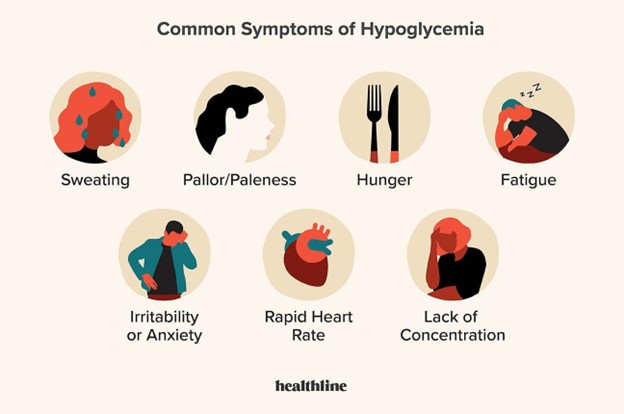
The nurse should teach a diabetic client that which symptom is indicative of hypoglycemia?
A. Anorexia
Reason: Anorexia is not a symptom of hypoglycemia, but it may indicate a loss of appetite due to other causes such as nausea, infection, or depression.
B. Warm skin
Reason: Warm skin is not a symptom of hypoglycemia, but it may indicate a fever, inflammation, or infection.
C. Fruity breath
Reason: Fruity breath is not a symptom of hypoglycemia, but it may indicate ketoacidosis, which is a serious complication of hyperglycemia.
D. Nervousness
Reason: Nervousness is a symptom of hypoglycemia, as the low blood glucose level affects the brain and causes anxiety, irritability, confusion, and tremors.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Proctored Exam 3. Take the full exam now
Full Explanation
Choice A Reason: Anorexia is not a symptom of hypoglycemia, but it may indicate a loss of appetite due to other causes such as nausea, infection, or depression.
Choice B Reason: Warm skin is not a symptom of hypoglycemia, but it may indicate a fever, inflammation, or infection.
Choice C Reason: Fruity breath is not a symptom of hypoglycemia, but it may indicate ketoacidosis, which is a serious complication of hyperglycemia.
Choice D Reason: Nervousness is a symptom of hypoglycemia, as the low blood glucose level affects the brain and causes anxiety, irritability, confusion, and tremors.
Similar Questions
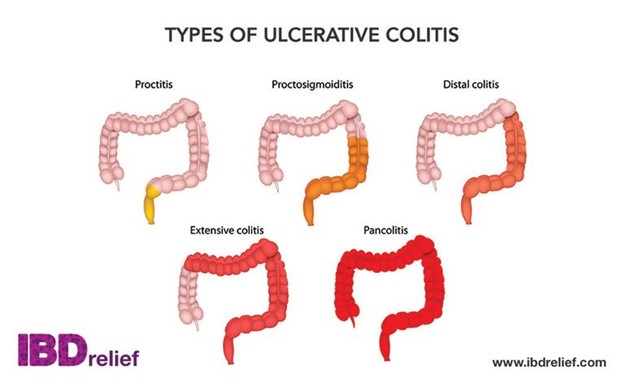
Which goal for the client's care should take priority when caring for a client admitted due to exacerbation of ulcerative colitis?
A. Managing diarrhea
Reason: Managing diarrhea is the priority goal for the client's care, as it helps to prevent dehydration, electrolyte imbalance, malnutrition, and infection.
B. Promoting rest and comfort
Reason: Promoting rest and comfort is an important goal for the client's care, but it is not the priority, as it does not address the underlying cause of the exacerbation.
C. Increasing self-esteem
Reason: Increasing self-esteem is a long-term goal for the client's care, but it is not the priority, as it does not affect the physical condition of the client.
D. Promoting self-care and independence
Reason: Promoting self-care and independence is a long-term goal for the client's care, but it is not the priority, as it does not affect the acute symptoms of the exacerbation.
Full Explanation
Choice A Reason: Managing diarrhea is the priority goal for the client's care, as it helps to prevent dehydration, electrolyte imbalance, malnutrition, and infection.
Choice B Reason: Promoting rest and comfort is an important goal for the client's care, but it is not the priority, as it does not address the underlying cause of the exacerbation.
Choice C Reason: Increasing self-esteem is a long-term goal for the client's care, but it is not the priority, as it does not affect the physical condition of the client.
Choice D Reason: Promoting self-care and independence is a long-term goal for the client's care, but it is not the priority, as it does not affect the acute symptoms of the exacerbation.
A client has been diagnosed with hypothyroidism. What information should the nurse obtain when conducting a focused assessment? Select all that apply.
A. Weight gain
Choice A Reason: Weight gain is a common finding in hypothyroidism, as the decreased thyroid hormone level causes the metabolism to slow down and the body to store more fat.
B. Constipation
Choice B Reason: Constipation is a common finding in hypothyroidism, as the decreased thyroid hormone level causes the gastrointestinal motility to decrease and the stools to become hard and dry.
C. Rapid pulse
Choice C Reason: Rapid pulse is not a common finding in hypothyroidism, but it may indicate other conditions such as hyperthyroidism or anxiety.
D. Decreased energy
Choice D Reason: Decreased energy is a common finding in hypothyroidism, as the decreased thyroid hormone level causes the body to feel tired and sluggish.
E. Hypertension
Choice E Reason: Hypertension is not a common finding in hypothyroidism, but it may indicate other conditions such as renal disease or cardiovascular disease.
Full Explanation
Choice A Reason: Weight gain is a common finding in hypothyroidism, as the decreased thyroid hormone level causes the metabolism to slow down and the body to store more fat.
Choice B Reason: Constipation is a common finding in hypothyroidism, as the decreased thyroid hormone level causes the gastrointestinal motility to decrease and the stools to become hard and dry.
Choice C Reason: Rapid pulse is not a common finding in hypothyroidism, but it may indicate other conditions such as hyperthyroidism or anxiety.
Choice D Reason: Decreased energy is a common finding in hypothyroidism, as the decreased thyroid hormone level causes the body to feel tired and sluggish.
Choice E Reason: Hypertension is not a common finding in hypothyroidism, but it may indicate other conditions such as renal disease or cardiovascular disease.
A client with multiple sclerosis is seen by the home health nurse and complains of severe fatigue. Which of the following is the most appropriate nursing intervention?
A. Encourage deep-breathing exercises
Reason: Encouraging deep-breathing exercises is not the most appropriate nursing intervention, as it may not reduce fatigue and may increase respiratory effort.
B. Provide a relaxing warm bath
Reason: Providing a relaxing warm bath is not the most appropriate nursing intervention, as it may worsen fatigue and increase the risk of heat intolerance and dehydration.
C. Schedule periods of rest in between activities
Reason: Scheduling periods of rest in between activities is the most appropriate nursing intervention, as it helps to conserve energy, prevent exhaustion, and promote recovery.
D. Administer multivitamins
Reason: Administering multivitamins is not the most appropriate nursing intervention, as it may not improve fatigue and may cause adverse effects or interactions with other medications.
Full Explanation
Choice A Reason: Encouraging deep-breathing exercises is not the most appropriate nursing intervention, as it may not reduce fatigue and may increase respiratory effort.
Choice B Reason: Providing a relaxing warm bath is not the most appropriate nursing intervention, as it may worsen fatigue and increase the risk of heat intolerance and dehydration.
Choice C Reason: Scheduling periods of rest in between activities is the most appropriate nursing intervention, as it helps to conserve energy, prevent exhaustion, and promote recovery.
Choice D Reason: Administering multivitamins is not the most appropriate nursing intervention, as it may not improve fatigue and may cause adverse effects or interactions with other medications.