Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
The prenatal clinic nurse monitored women for preeclampsia. All four women were in the clinic at the same time. Which one should the nurse see first?
A. Weight gain of 0.5 kg during the past 2 weeks
Choice A) Weight gain of 0.5 kg during the past 2 weeks: This is a normal weight gain for a pregnant woman and does not indicate preeclampsia.
B. Pitting pedal edema at the end of the day
Choice B) Pitting pedal edema at the end of the day: This is a common symptom of pregnancy and does not necessarily indicate preeclampsia. It can be relieved by elevating the legs and wearing compression stockings.
C. Blood pressure increase to 138/86 mm Hg
Choice C) Blood pressure increases to 138/86 mm Hg: This is a mild elevation of blood pressure and does not meet the criteria for preeclampsia, which is defined as a systolic blood pressure of 140 mm Hg or higher or a diastolic blood pressure of 90 mm Hg or higher on two occasions at least four hours apart.
D. Dipstick value of 3+ for protein in her urine
Choice D) Dipstick value of 3+ for protein in her urine: This is a sign of significant proteinuria, which is one of the main features of preeclampsia. Proteinuria is defined as a urinary protein excretion of 300 mg or more in 24 hours or a dipstick reading of 1+ or higher. A dipstick value of 3+ indicates severe proteinuria and requires immediate attention and treatment. This woman has the highest risk of developing complications from preeclampsia, such as eclampsia, HELLP syndrome, placental abruption, or fetal growth restriction. Therefore, she should be seen by the nurse first.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Maternity Proctored Exam 2. Take the full exam now
Full Explanation
Choice A) Weight gain of 0.5 kg during the past 2 weeks: This is a normal weight gain for a pregnant woman and does not indicate preeclampsia.
Choice B) Pitting pedal edema at the end of the day: This is a common symptom of pregnancy and does not necessarily indicate preeclampsia. It can be relieved by elevating the legs and wearing compression stockings.
Choice C) Blood pressure increase to 138/86 mm Hg: This is a mild elevation of blood pressure and does not meet the criteria for preeclampsia, which is defined as a systolic blood pressure of 140 mm Hg or higher or a diastolic blood pressure of 90 mm Hg or higher on two occasions at least four hours apart.
Choice D) Dipstick value of 3+ for protein in her urine: This is a sign of significant proteinuria, which is one of the main features of preeclampsia. Proteinuria is defined as a urinary protein excretion of 300 mg or more in 24 hours or a dipstick reading of 1+ or higher. A dipstick value of 3+ indicates severe proteinuria and requires immediate attention and treatment. This woman has the highest risk of developing complications from preeclampsia, such as eclampsia, HELLP syndrome, placental abruption, or fetal growth restriction . Therefore, she should be seen by the nurse first.

Similar Questions
A woman is in active labor. On spontaneous rupture of her membranes, the nurse caring for this woman notices variable deceleration patterns during evaluation of the monitor tracing. When preparing to perform a vaginal examination, the nurse observes a small section of the umbilical cord protruding from the vagina. What should the nurse do next?
A. Wrap the cord loosely with a sterile towel saturated with warm normal saline.
Choice A) Wrap the cord loosely with a sterile towel saturated with warm normal saline: This is not an appropriate action because it does not relieve the compression of the cord, which can cause fetal hypoxia and acidosis. The cord should be kept moist, but not wrapped around anything.
B. Place a sterile gloved hand into the vagina and hold the presenting part off the cord while calling for assistance.
Choice B) Place a sterile gloved hand into the vagina and hold the presenting part off the cord while calling for assistance: This is the correct action because it prevents further descent of the fetus and reduces the pressure on the cord, which can improve fetal oxygenation and blood flow. The nurse should also elevate the woman's hips and place her in a knee-chest or Trendelenburg position to reduce gravity. The nurse should call for immediate assistance and prepare for an emergency cesarean section.
C. Increase the IV drip rate.
Choice C) Increase the IV drip rate: This is not an appropriate action because it does not address the cause of the variable decelerations, which is cord compression. Increasing the IV fluid may cause fluid overload and worsen maternal and fetal outcomes.
D. Administer oxygen to the woman via mask at 8 to 10 L/minute.
Choice D) Administer oxygen to the woman via mask at 8 to 10 L/minute: This is not an appropriate action because it does not relieve the cord compression, which is the main threat to fetal well-being. Oxygen administration may be helpful in some cases of fetal distress, but it is not sufficient in this situation.
Full Explanation
Choice A) Wrap the cord loosely with a sterile towel saturated with warm normal saline: This is not an appropriate action because it does not relieve the compression of the cord, which can cause fetal hypoxia and acidosis. The cord should be kept moist, but not wrapped around anything.
Choice B) Place a sterile gloved hand into the vagina and hold the presenting part off the cord while calling for assistance: This is the correct action because it prevents further descent of the fetus and reduces the pressure on the cord, which can improve fetal oxygenation and blood flow. The nurse should also elevate the woman's hips and place her in a knee-chest or Trendelenburg position to reduce gravity. The nurse should call for immediate assistance and prepare for an emergency cesarean section.
Choice C) Increase the IV drip rate: This is not an appropriate action because it does not address the cause of the variable decelerations, which is cord compression. Increasing the IV fluid may cause fluid overload and worsen maternal and fetal outcomes.
Choice D) Administer oxygen to the woman via mask at 8 to 10 L/minute: This is not an appropriate action because it does not relieve the cord compression, which is the main threat to fetal well-being. Oxygen administration may be helpful in some cases of fetal distress, but it is not sufficient in this situation.
A newborn has meconium aspiration at birth. The nurse notes increasing respiratory distress. What action takes priority?
A. Obtain an oxygen saturation.
Choice A) Obtain an oxygen saturation: This is not a priority action because it does not address the underlying cause of the respiratory distress, which is meconium aspiration. Meconium aspiration can cause airway obstruction, inflammation, infection, and pulmonary hypertension in the newborn. Oxygen saturation may be low, but it is not a reliable indicator of the severity of the condition.
B. Stimulate the baby to increase respirations.
Choice B) Stimulate the baby to increase respirations: This is not a priority action because it may worsen the respiratory distress by increasing the work of breathing and causing more meconium to be aspirated. Stimulation may also cause stress and hypoxia in the newborn.
C. Prepare to initiate ECMO.
Choice C) Prepare to initiate ECMO: This is not a priority action because it is a last resort treatment for severe cases of meconium aspiration syndrome that do not respond to conventional therapies. ECMO stands for extracorporeal membrane oxygenation, which is a form of life support that bypasses the lungs and provides oxygen to the blood. ECMO has many risks and complications, such as bleeding, infection, and organ damage. It should only be used when other options have failed and with the consent of the parents.
D. Notify the provider at once.
Choice D) Notify the provider at once: This is the correct action because it allows for prompt assessment and intervention by the provider, who can initiate appropriate treatments for meconium aspiration syndrome. These may include suctioning of the airway, administration of antibiotics, surfactant, or inhaled nitric oxide, and mechanical ventilation . Early treatment can improve the outcomes and reduce the complications of meconium aspiration syndrome.
Full Explanation
Choice A) Obtain an oxygen saturation: This is not a priority action because it does not address the underlying cause of the respiratory distress, which is meconium aspiration. Meconium aspiration can cause airway obstruction, inflammation, infection, and pulmonary hypertension in the newborn. Oxygen saturation may be low, but it is not a reliable indicator of the severity of the condition.
Choice B) Stimulate the baby to increase respirations: This is not a priority action because it may worsen the respiratory distress by increasing the work of breathing and causing more meconium to be aspirated. Stimulation may also cause stress and hypoxia in the newborn.
Choice C) Prepare to initiate ECMO: This is not a priority action because it is a last resort treatment for severe cases of meconium aspiration syndrome that do not respond to conventional therapies. ECMO stands for extracorporeal membrane oxygenation, which is a form of life support that bypasses the lungs and provides oxygen to the blood.
ECMO has many risks and complications, such as bleeding, infection, and organ damage. It should only be used when other options have failed and with the consent of the parents.
Choice D) Notify the provider at once: This is the correct action because it allows for prompt assessment and intervention by the provider, who can initiate appropriate treatments for meconium aspiration syndrome. These may include suctioning of the airway, administration of antibiotics, surfactant, or inhaled nitric oxide, and mechanical ventilation . Early treatment can improve the outcomes and reduce the complications of meconium aspiration syndrome.

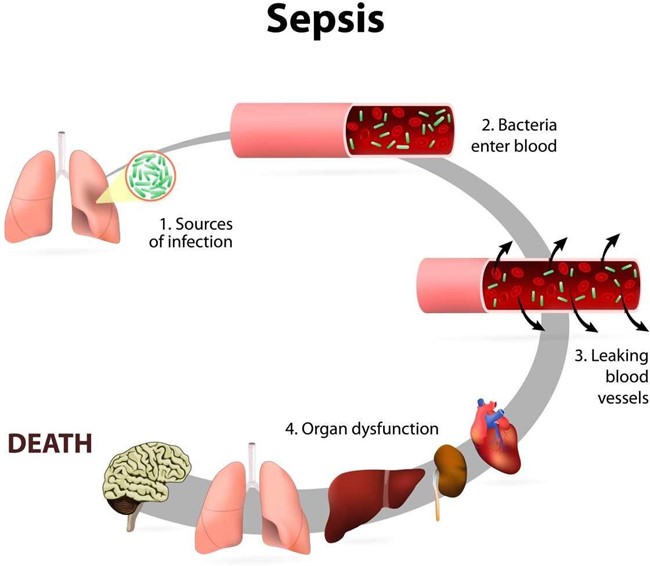
Which of the following would the nurse expect to assess in a newborn who develops sepsis?
A. Increased urinary output
Choice A) Increased urinary output: This is not a sign of sepsis in newborns. In fact, sepsis can cause reduced urinary output due to poor blood flow to the kidneys and dehydration.
B. Hypothermia
Choice B) Hypothermia: This is a sign of sepsis in newborns. Sepsis can cause changes in temperature, often fever, but sometimes low temperature. Hypothermia can indicate a severe infection that affects the body's ability to regulate its temperature.
C. Wakefulness
Choice C) Wakefulness: This is not a sign of sepsis in newborns. Sepsis can cause reduced activity and lethargy due to inflammation and organ dysfunction.
D. Interest in feeding
Choice D) Interest in feeding: This is not a sign of sepsis in newborns. Sepsis can cause reduced sucking and difficulty feeding due to poor appetite, nausea, vomiting, and abdominal distension.
Full Explanation
Choice A) Increased urinary output: This is not a sign of sepsis in newborns. In fact, sepsis can cause reduced urinary output due to poor blood flow to the kidneys and dehydration.
Choice B) Hypothermia: This is a sign of sepsis in newborns. Sepsis can cause changes in temperature, often fever, but sometimes low temperature. Hypothermia can indicate a severe infection that affects the body's ability to regulate its temperature.
Choice C) Wakefulness: This is not a sign of sepsis in newborns. Sepsis can cause reduced activity and lethargy due to inflammation and organ dysfunction.
Choice D) Interest in feeding: This is not a sign of sepsis in newborns. Sepsis can cause reduced sucking and difficulty feeding due to poor appetite, nausea, vomiting, and abdominal distension.