Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
The registered nurse is preparing for the termination phase of the nurse-client relationship. The registered nurse prepares to implement which nursing task that is most appropriate and most important for this phase?
Select one:
A. Developing realistic solutions
Option a. Developing realistic solutions is an important task during the working phase of the nurse-client relationship, when the nurse and client work together to identify and implement solutions to the client’s problems.
B. Built rapport and trust.
Option b. Building rapport and trust is an important task during the orientation phase of the nurse-client relationship, when the nurse and client get to know each other and establish a therapeutic relationship.
C. Making appropriate referrals
During the termination phase of the nurse-client relationship, the nurse should focus on making appropriate referrals to ensure that the client continues to receive the care and support they need after the relationship with the nurse has ended.
D. Identifying expected outcomes
Option d. Identifying expected outcomes is an important task during the planning phase of the nursing process, when the nurse and client work together to set goals and develop a plan of care.
This question is an excerpt from Nurse Dive's nursing test bank - Mental Health - Proctored Exam 2. Take the full exam now
Full Explanation
During the termination phase of the nurse-client relationship, the nurse should focus on making appropriate referrals to ensure that the client continues to receive the care and support they need after the relationship with the nurse has ended.
Option a. Developing realistic solutions is an important task during the working phase of the nurse-client relationship, when the nurse and client work together to identify and implement solutions to the client’s problems.
Option b. Building rapport and trust is an important task during the orientation phase of the nurse-client relationship, when the nurse and client get to know each other and establish a therapeutic relationship.
Option d. Identifying expected outcomes is an important task during the planning phase of the nursing process, when the nurse and client work together to set goals and develop a plan of care.
Similar Questions
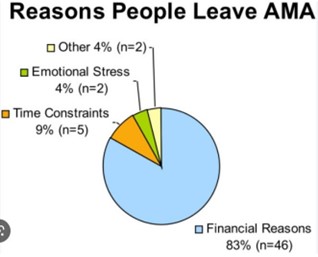
An involuntarily hospitalized client tells the nurse: "Get me the forms for discharge against medical advice (AMA) so I leave the hospital now." What is the registered nurse's best initial response?
Select one:
A. "l will get them for you. but let's talk about your decision to leave treatment."
This response acknowledges the client's request for the forms while also addressing the need to discuss the client's decision to leave treatment. It provides an opportunity for the nurse to explore the client's reasons for wanting to leave, discuss the potential consequences of leaving against medical advice, and address any concerns or fears the client may have about continuing treatment.
B. 'Since you signed your consent for treatment, you may leave if you desire, it is ok."
Option b is not appropriate because it does not address the potential risks associated with leaving treatment against medical advice.
C. “l can’t give you those forms without your health care provider's knowledge."
Option c is also not appropriate because it does not acknowledge the client's request and is potentially misleading.
D. "I'll get the forms for you right now and bring them to your room."
Option d is not appropriate because it does not address the client's reasons for wanting to leave or the potential consequences of leaving against medical advice.
Full Explanation
This response acknowledges the client's request for the forms while also addressing the need to discuss the client's decision to leave treatment. It provides an opportunity for the nurse to explore the client's reasons for wanting to leave, discuss the potential consequences of leaving against medical advice, and address any concerns or fears the client may have about continuing treatment.
Option b is not appropriate because it does not address the potential risks associated with leaving treatment against medical advice.
Option c is also not appropriate because it does not acknowledge the client's request and is potentially misleading.
Option d is not appropriate because it does not address the client's reasons for wanting to leave or the potential consequences of leaving against medical advice.
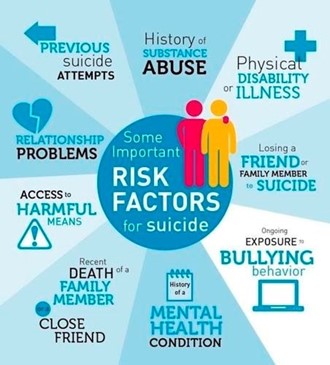
A registered nurse is providing a community health education class about suicide prevention. Which of the following should the nurse identify as risk factors for suicide? (Select all that apply).
A. Substance abuse disorder
Option a. Substance abuse disorder can increase the risk of suicide because it can exacerbate underlying mental health conditions and impair judgment.
B. Schizophrenia
Option b. Schizophrenia is a mental health condition that can increase the risk of suicide due to symptoms such as delusions and hallucinations.
C. Age greater than 55 years Old
Option c. Age greater than 55 years old is a risk factor for suicide because older adults may experience social isolation, chronic health conditions, and loss of independence.
D. Female gender
Option d. Female gender is not a known risk factor for suicide.
F. Male gender
Option f. Male gender is a risk factor for suicide because men are more likely to die by suicide than women.
G. Bachelor’s degree
Option g. Having a bachelor’s degree is not a known risk factor for suicide.
H. Previous suicide attempt.
Option h. Previous suicide attempt is a strong predictor of future suicide attempts and completed suicides.
Full Explanation
a. Substance abuse disorder
b. Schizophrenia
c. Age greater than 55 years old
f. Male gender
h. Previous suicide attempt.
Option a. Substance abuse disorder can increase the risk of suicide because it can exacerbate underlying mental health conditions and impair judgment.
Option b. Schizophrenia is a mental health condition that can increase the risk of suicide due to symptoms such as delusions and hallucinations.
Option c. Age greater than 55 years old is a risk factor for suicide because older adults may experience social isolation, chronic health conditions, and loss of independence.
Option f. Male gender is a risk factor for suicide because men are more likely to die by suicide than women. Option h. Previous suicide attempt is a strong predictor of future suicide attempts and completed suicides. Option d. Female gender is not a known risk factor for suicide.
Option e. Being currently married is not a known risk factor for suicide. Option g. Having a bachelor’s degree is not a known risk factor for suicide.
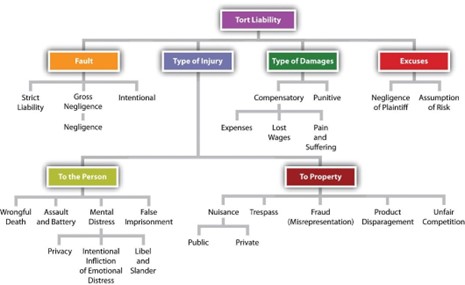
A registered nurse puts a client who has a psychotic disorder in seclusion overnight because the unit is very short-staffed, and the client frequently fights with other clients. the nurse's actions are an example of which of the following torts?
A. Invasion of privacy
Option a. Invasion of privacy refers to the violation of a person’s right to privacy.
B. Battery
Option b. Battery refers to the intentional and harmful or offensive touching of another person without their consent.
C. False imprisonment
False imprisonment is the unlawful restraint of a person against their will. In this situation, the nurse’s actions of placing the client in seclusion overnight because the unit is short-staffed and the client frequently fights with other clients may be considered false imprisonment if the client did not consent to being placed in seclusion and if there were no legal grounds for doing so.
D. Assault
Option d. Assault refers to the intentional act of causing another person to fear immediate harm or offensive contact.
Full Explanation
False imprisonment is the unlawful restraint of a person against their will. In this situation, the nurse’s actions of placing the client in seclusion overnight because the unit is short-staffed and the client frequently fights with other clients may be considered false imprisonment if the client did not consent to being placed in seclusion and if there were no legal grounds for doing so.
Option a. Invasion of privacy refers to the violation of a person’s right to privacy.
Option b. Battery refers to the intentional and harmful or offensive touching of another person without their consent.
Option d. Assault refers to the intentional act of causing another person to fear immediate harm or offensive contact.