Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
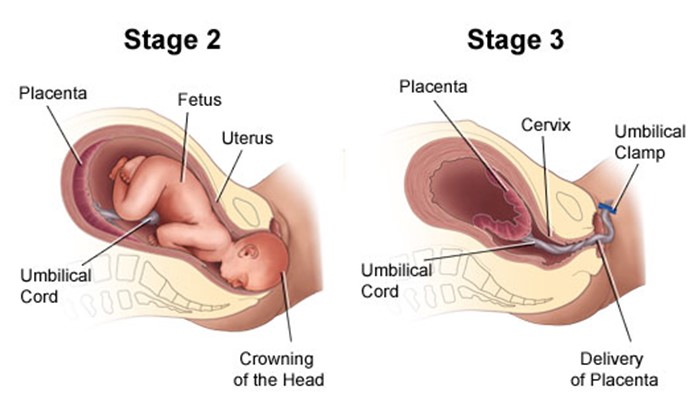
What nursing intervention is particularly indicated for the second stage of labor?
A. Providing pain medication to increase the client's tolerance of labor pains
Providing pain medication to increase the client's tolerance of labor pains is not a specific intervention for the second stage of labor. Pain medication is a drug that relieves pain by blocking pain signals or reducing inflammation. Pain medication can be given during any stage of labor, depending on the client's preference and condition. However, pain medication may have side effects such as sedation, nausea, or respiratory depression, and may affect the fetal heart rate or the progress of labor.
B. Assessing the fetal heart rate and pattern for signs of fetal distress
Assessing the fetal heart rate and pattern for signs of fetal distress is not a particular intervention for the second stage of labor. Fetal heart rate and pattern are indicators of fetal well-being and oxygenation. Fetal heart rate and pattern should be monitored throughout labor, especially during contractions, to detect any abnormalities or complications such as bradycardia, tachycardia, or decelerations.
C. Assisting the client to push effectively so that expulsion of the fetus can be achieved
This is the correct answer because assisting the client to push effectively so that expulsion of the fetus can be achieved is a vital intervention for the second stage of labor. The second stage of labor begins when the cervix is fully dilated (10 cm) and ends with the delivery of the baby. The nurse should coach the client to push with each contraction, using proper breathing and positioning techniques, and provide feedback and encouragement.
D. Monitoring effects of oxytocin administration to help achieve cervical dilation
Monitoring effects of oxytocin administration to help achieve cervical dilation is not a relevant intervention for the second stage of labor. Oxytocin is a hormone that stimulates uterine contractions and cervical dilation. Oxytocin can be administered during labor to augment or induce labor, especially if there is prolonged or dysfunctional labor. However, oxytocin is not needed in the second stage of labor, when the cervix is already fully dilated and the focus is on pushing and delivering the baby.
This question is an excerpt from Nurse Dive's nursing test bank - HESI Exit II Proctored Exam. Take the full exam now
Full Explanation
Choice A reason: Providing pain medication to increase the client's tolerance of labor pains is not a specific intervention for the second stage of labor. Pain medication is a drug that relieves pain by blocking pain signals or reducing inflammation. Pain medication can be given during any stage of labor, depending on the client's preference and condition. However, pain medication may have side effects such as sedation, nausea, or respiratory depression, and may affect the fetal heart rate or the progress of labor.
Choice B reason: Assessing the fetal heart rate and pattern for signs of fetal distress is not a particular intervention for the second stage of labor. Fetal heart rate and pattern are indicators of fetal well-being and oxygenation. Fetal heart rate and pattern should be monitored throughout labor, especially during contractions, to detect any abnormalities or complications such as bradycardia, tachycardia, or decelerations.
Choice D reason: Monitoring effects of oxytocin administration to help achieve cervical dilation is not a relevant intervention for the second stage of labor. Oxytocin is a hormone that stimulates uterine contractions and cervical dilation. Oxytocin can be administered during labor to augment or induce labor, especially if there is prolonged or dysfunctional labor. However, oxytocin is not needed in the second stage of labor, when the cervix is already fully dilated and the focus is on pushing and delivering the baby.
Similar Questions
The healthcare provider prescribes and IV solution of regular insulin (Humulin-R) 100 units in 250 ml of 0.45% saline to infuse at 12 units/hour. The nurse should program the infusion pump to deliver how many ml/hour?
Full Explanation
First, we need to find the concentration of insulin in the IV solution, which is the ratio of insulin units to saline volume. To do this, we use the given information that the IV solution contains 100 units in 250 ml. So, we divide 100 by 250 and get 0.4 units/ml.
Next, we need to calculate the infusion rate in ml/hour for the ordered dose of 12 units/hour. To do this, we use the ratio of insulin units to saline volume, which is 0.4 units/ml. So, we set up a proportion as follows:
0.4/1=12/x
To solve for x, we cross-multiply and get 0.4 x = 12. Then, we divide both sides by 0.4 and get x = 30. So, the infusion rate is 30 ml/hour.
Therefore, the nurse should program the infusion pump to deliver 30 ml/hour..
A preschool-aged child who is being tested for Streptococcal pharyngitis returns to the clinic for signs of scarlet fever. Which assessment finding
provides the clearest indication to the nurse that the child is experiencing a reaction to toxins that are created by Streptococcal bacteria.
A. Flushed, peeling skin
Flushed, peeling skin is a classic sign of scarlet fever, which is a condition that can arise from Streptococcal pharyngitis. Scarlet fever is characterized by a red rash that can cover most of the body and may lead to the skin peeling. This symptom is a direct reaction to the toxins produced by the Streptococcal bacteria.
B. Red bumps across chest
Red bumps across the chest could be indicative of many conditions and are not specifically characteristic of the reaction to toxins produced by Streptococcal bacteria. While a rash is common in scarlet fever, it typically starts on the face or neck and spreads to the rest of the body, rather than presenting as isolated red bumps.
C. White coating on tongue
A white coating on the tongue, often referred to as “strawberry tongue,” is indeed associated with scarlet fever. However, it is not the clearest indication of a reaction to the toxins. The white coating usually precedes the strawberry-like appearance, where the tongue becomes red and bumpy.
D. High, protracted fever
While a high fever is a symptom of scarlet fever, it is not specific to the reaction to toxins from Streptococcal bacteria, as many infections can cause high fevers. The term “protracted” suggests a prolonged fever, which could be seen in various conditions.
Full Explanation
The correct answer is A. Flushed, peeling skin
Choice A reason: Flushed, peeling skin is a classic sign of scarlet fever, which is a condition that can arise from Streptococcal pharyngitis. Scarlet fever is characterized by a red rash that can cover most of the body and may lead to the skin peeling. This symptom is a direct reaction to the toxins produced by the Streptococcal bacteria.
Choice B reason: Red bumps across the chest could be indicative of many conditions and are not specifically characteristic of the reaction to toxins produced by Streptococcal bacteria. While a rash is common in scarlet fever, it typically starts on the face or neck and spreads to the rest of the body, rather than presenting as isolated red bumps.
Choice C reason: A white coating on the tongue, often referred to as “strawberry tongue,” is indeed associated with scarlet fever. However, it is not the clearest indication of a reaction to the toxins. The white coating usually precedes the strawberry-like appearance, where the tongue becomes red and bumpy.
Choice D reason: While a high fever is a symptom of scarlet fever, it is not specific to the reaction to toxins from Streptococcal bacteria, as many infections can cause high fevers. The term “protracted” suggests a prolonged fever, which could be seen in various conditions.
The nurse is caring for a client who arrives to the emergency department with reports of experiencing dizziness and difficulty walking to the bathroom.
The nurse observes right-sided weakness and sluggish enunciation of speech. The nurse should immediately take which action?
A. Keep the bed in the lowest position and initiate seizure and fall precautions.
Keeping the bed in the lowest position and initiating seizure and fall precautions is not an immediate action for the nurse to take. Seizure and fall precautions are measures that prevent injury or harm to the client in case of a seizure or a fall. Seizure and fall precautions include lowering the bed, padding the side rails, removing any objects that may cause injury, and having suction and oxygen equipment ready. However, these precautions are not specific to the client's condition and do not address the underlying cause.
B. Place an indwelling urinary catheter and measure strict intake and output.
Placing an indwelling urinary catheter and measuring strict intake and output is not an urgent action for the nurse to take. An indwelling urinary catheter is a tube that drains urine from the bladder into a collection bag. Measuring intake and output is a way of monitoring fluid balance and kidney function. However, these interventions are not essential for the client's condition and may increase the risk of infection or trauma.
C. Maintain elevated positioning of the dependent joints on affected side.
Maintaining elevated positioning of the dependent joints on affected side is not a relevant action for the nurse to take. Dependent joints are joints that are below the level of the heart, such as the ankles or wrists. Elevating dependent joints can help reduce swelling or pain by improving blood flow and drainage. However, this intervention is not related to the client's condition and does not improve neurological function.
D. Start two large bore IV catheters and review inclusion criteria for IV fibrinolytic therapy.
Full Explanation
Choice A reason: Keeping the bed in the lowest position and initiating seizure and fall precautions is not an immediate action for the nurse to take. Seizure and fall precautions are measures that prevent injury or harm to the client in case of a seizure or a fall. Seizure and fall precautions include lowering the bed, padding the side rails, removing any objects that may cause injury, and having suction and oxygen equipment ready. However, these precautions are not specific to the client's condition and do not address the underlying cause.
Choice B reason: Placing an indwelling urinary catheter and measuring strict intake and output is not an urgent action for the nurse to take. An indwelling urinary catheter is a tube that drains urine from the bladder into a collection bag. Measuring intake and output is a way of monitoring fluid balance and kidney function. However, these interventions are not essential for the client's condition and may increase the risk of infection or trauma.
Choice C reason: Maintaining elevated positioning of the dependent joints on affected side is not a relevant action for the nurse to take. Dependent joints are joints that are below the level of the heart, such as the ankles or wrists. Elevating dependent joints can help reduce swelling or pain by improving blood flow and drainage. However, this intervention is not related to the client's condition and does not improve neurological function.