Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
When is it most important for the nurse to assess a pregnant client's deep tendon reflexes (DTRs)?
A. When the client has ankle edema.
When the client has ankle edema, it is important for the nurse to assess for other signs of fluid retention, such as weight gain, jugular venous distension, and crackles in the lungs. However, ankle edema alone is not a specific indicator of preeclampsia or eclampsia, which are conditions that can cause hyperreflexia or increased DTRs.
B. If the client has an elevated blood pressure.
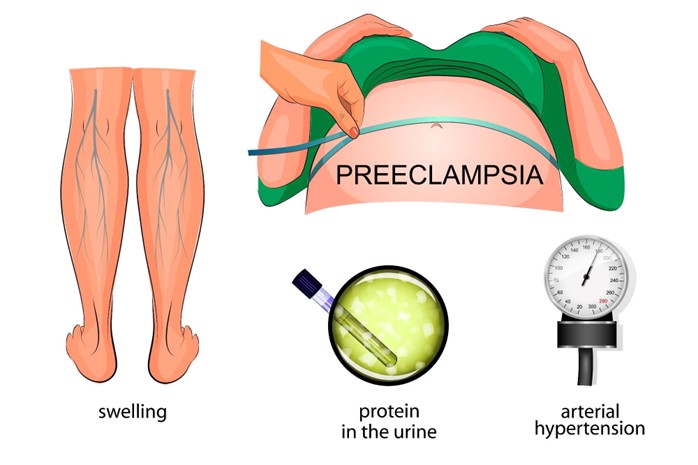
This is the correct answer because if the client has elevated blood pressure, it is important for the nurse to assess for other signs of preeclampsia or eclampsia, such as proteinuria, headache, blurred vision, epigastric pain, and hyperreflexia or increased DTRs. These conditions can cause seizures and other complications that can endanger the mother and fetus.
C. During admission to labor and delivery.
During admission to labor and delivery, it is important for the nurse to assess various aspects of the client's health status, such as vital signs, fetal heart rate, contractions, cervical dilation, and pain level. However, assessing DTRs is not a routine part of labor and delivery assessment unless there are signs of preeclampsia or eclampsia.
D. Within the first trimester of pregnancy.
Within the first trimester of pregnancy, it is important for the nurse to assess for signs of pregnancy-related nausea and vomiting, bleeding, infection, and ectopic pregnancy. However, assessing DTRs is not a routine part of first trimester assessment unless there are signs of neurological disorders or spinal cord injury.
This question is an excerpt from Nurse Dive's nursing test bank - HESI Exit II Proctored Exam. Take the full exam now
Full Explanation
Choice A reason: When the client has ankle edema, it is important for the nurse to assess for other signs of fluid retention, such as weight gain, jugular venous distension, and crackles in the lungs. However, ankle edema alone is not a specific indicator of preeclampsia or eclampsia, which are conditions that can cause hyperreflexia or increased DTRs.
Choice C reason: During admission to labor and delivery, it is important for the nurse to assess various aspects of the client's health status, such as vital signs, fetal heart rate, contractions, cervical dilation, and pain level. However, assessing DTRs is not a routine part of labor and delivery assessment unless there are signs of preeclampsia or eclampsia.
Choice D reason: Within the first trimester of pregnancy, it is important for the nurse to assess for signs of pregnancy-related nausea and vomiting, bleeding, infection, and ectopic pregnancy. However, assessing DTRs is not a routine part of first trimester assessment unless there are signs of neurological disorders or spinal cord injury.
Similar Questions
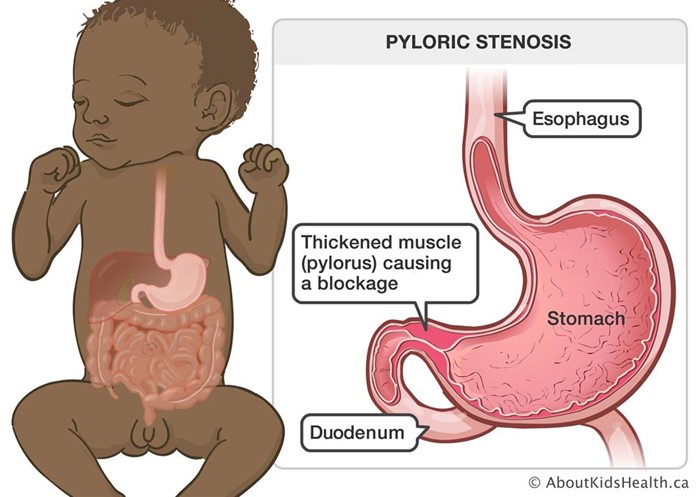
A 6-week-old infant with pyloric stenosis is scheduled for a pyloromyotomy. Which pre-operative nursing action has the highest priority?
A. Mark an outline of the "olive-shaped" mass in the right epigastric area.
Marking an outline of the "olive-shaped" mass in the right epigastric area is not a priority nursing action. The mass is caused by hypertrophy of the pyloric sphincter, which obstructs gastric emptying and causes projectile vomiting. The mass may not be palpable in all cases.
B. Instruct parents regarding care of the incisional area.
Instructing parents regarding care of the incisional area is a post-operative nursing action, not a pre-operative one. The parents will need to learn how to keep the incision clean and dry, monitor for signs of infection, and administer pain medication as prescribed.
C. Monitor amount of intake and infant's response to feedings.
Monitoring amount of intake and infant's response to feedings is important, but not the highest priority. The infant may have difficulty feeding due to nausea, vomiting, and abdominal pain.
D. Initiate a continuous infusion of IV fluids per prescription.
This is the correct answer because initiating a continuous infusion of IV fluids per prescription is essential to prevent dehydration and electrolyte imbalance in the infant. The infant may have significant fluid loss due to vomiting and poor intake.
Full Explanation
Choice A reason: Marking an outline of the "olive-shaped" mass in the right epigastric area is not a priority nursing action. The mass is caused by hypertrophy of the pyloric sphincter, which obstructs gastric emptying and causes projectile vomiting. The mass may not be palpable in all cases.
Choice B reason: Instructing parents regarding care of the incisional area is a post-operative nursing action, not a pre-operative one. The parents will need to learn how to keep the incision clean and dry, monitor for signs of infection, and administer pain medication as prescribed.
Choice C reason: Monitoring amount of intake and infant's response to feedings is important, but not the highest priority. The infant may have difficulty feeding due to nausea, vomiting, and abdominal pain.
The nurse is assessing a first day postpartum client. Which finding is most indicative of a postpartum infection?
White Blood Cell (WBC. Reference Range: 5000-10,000/mm^3 (5-10 x 10^9/L)
A. Moderate amount of foul-smelling lochia.
B. Blood pressure of 122/74 mm Hg
Blood pressure of 122/74 mm Hg is within the normal range for a postpartum client and does not indicate an infection. However, the nurse should monitor for signs of preeclampsia or eclampsia, such as hypertension, proteinuria, headache, blurred vision, and seizures.
C. Oral temperature of 100.2°F (37.9°C..
Oral temperature of 100.2°F (37.9°C. is slightly elevated, but not necessarily indicative of an infection. A mild fever may occur within the first 24 hours after delivery due to dehydration or hormonal changes. However, if the fever persists or increases, the nurse should suspect an infection and notify the healthcare provider.
D. White blood cell count of 19,000/mm^3 (19 x 10^9/L)
White blood cell count of 19,000/mm^3 (19 x 10^9/L) is higher than the normal range, but not necessarily indicative of an infection. A leukocytosis or increased WBC count may occur as a normal response to stress or trauma during delivery. However, if the WBC count remains elevated or increases further, the nurse should suspect an infection and notify the healthcare provider.
Full Explanation
Choice B reason: Blood pressure of 122/74 mm Hg is within the normal range for a postpartum client and does not indicate an infection. However, the nurse should monitor for signs of preeclampsia or eclampsia, such as hypertension, proteinuria, headache, blurred vision, and seizures.
Choice C reason: Oral temperature of 100.2°F (37.9°C. is slightly elevated, but not necessarily indicative of an infection. A mild fever may occur within the first 24 hours after delivery due to dehydration or hormonal changes. However, if the fever persists or increases, the nurse should suspect an infection and notify the healthcare provider.
Choice D reason: White blood cell count of 19,000/mm^3 (19 x 10^9/L) is higher than the normal range, but not necessarily indicative of an infection. A leukocytosis or increased WBC count may occur as a normal response to stress or trauma during delivery. However, if the WBC count remains elevated or increases further, the nurse should suspect an infection and notify the healthcare provider.
A 6-week-old infant with pyloric stenosis is scheduled for a pyloromyotomy. Which pre-operative nursing action has the highest priority?
A. Mark an outline of the "olive-shaped" mass in the right epigastric area.
Marking an outline of the "olive-shaped" mass in the right epigastric area is not a priority nursing action. The mass is caused by hypertrophy of the pyloric sphincter, which obstructs gastric emptying and causes projectile vomiting. The mass may not be palpable in all cases.
B. Instruct parents regarding care of the incisional area.
Instructing parents regarding care of the incisional area is a post-operative nursing action, not a pre-operative one. The parents will need to learn how to keep the incision clean and dry, monitor for signs of infection, and administer pain medication as prescribed.
C. Monitor amount of intake and infant's response to feedings.
Monitoring amount of intake and infant's response to feedings is important, but not the highest priority. The infant may have difficulty feeding due to nausea, vomiting, and abdominal pain.
D. Initiate a continuous infusion of IV fluids per prescription.
None
Full Explanation
Choice A reason: Marking an outline of the "olive-shaped" mass in the right epigastric area is not a priority nursing action. The mass is caused by hypertrophy of the pyloric sphincter, which obstructs gastric emptying and causes projectile vomiting. The mass may not be palpable in all cases.
Choice B reason: Instructing parents regarding care of the incisional area is a post-operative nursing action, not a pre-operative one. The parents will need to learn how to keep the incision clean and dry, monitor for signs of infection, and administer pain medication as prescribed.
Choice C reason: Monitoring amount of intake and infant's response to feedings is important, but not the highest priority. The infant may have difficulty feeding due to nausea, vomiting, and abdominal pain.