Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A. Observe insertion site.
A: Observing insertion site is an essential assessment for a client who has a suprapubic catheter. The insertion site is located in the lower abdomen, where urine drains from an opening in the bladder through a catheter into a drainage bag. The nurse should inspect the site for signs of infection, inflammation, bleeding, or leakage. The nurse should also clean the site with soap and water and apply a sterile dressing as needed.
B. Palpate flank area.
B: Palpating flank area is not a relevant assessment for a client who has a suprapubic catheter. The flank area is located on the sides of the back, where the kidneys are located. Palpating the flank area can detect tenderness or pain that may indicate kidney infection or stones, but it does not provide information about the suprapubic catheter or its function.
C. Measure abdominal girth.
C: Measuring abdominal girth is not a relevant assessment for a client who has a suprapubic catheter. The abdominal girth is the circumference of the abdomen at the level of the umbilicus. Measuring abdominal girth can detect changes in fluid balance, ascites, or bowel obstruction, but it does not provide information about the suprapubic catheter or its function.
D. Assess perineal area.
D: Assessing perineal area is not a relevant assessment for a client who has a suprapubic catheter. The perineal area is located between the anus and the genitals. Assessing perineal area can detect signs of infection, irritation, or injury in the genital or anal regions, but it does not provide information about the suprapubic catheter or its function.
This question is an excerpt from Nurse Dive's nursing test bank - HESI Exit II Proctored Exam. Take the full exam now
Full Explanation
Choice A: Observing insertion site is an essential assessment for a client who has a suprapubic catheter. The insertion site is located in the lower abdomen, where urine drains from an opening in the bladder through a catheter into a drainage bag. The nurse should inspect the site for signs of infection, inflammation, bleeding, or leakage. The nurse should also clean the site with soap and water and apply a sterile dressing as needed.
Choice B: Palpating flank area is not a relevant assessment for a client who has a suprapubic catheter. The flank area is located on the sides of the back, where the kidneys are located. Palpating the flank area can detect tenderness or pain that may indicate kidney infection or stones, but it does not provide information about the suprapubic catheter or its function.
Choice C: Measuring abdominal girth is not a relevant assessment for a client who has a suprapubic catheter. The abdominal girth is the circumference of the abdomen at the level of the umbilicus. Measuring abdominal girth can detect changes in fluid balance, ascites, or bowel obstruction, but it does not provide information about the suprapubic catheter or its function.
Choice D: Assessing perineal area is not a relevant assessment for a client who has a suprapubic catheter. The perineal area is located between the anus and the genitals. Assessing perineal area can detect signs of infection, irritation, or injury in the genital or anal regions, but it does not provide information about the suprapubic catheter or its function.
Similar Questions
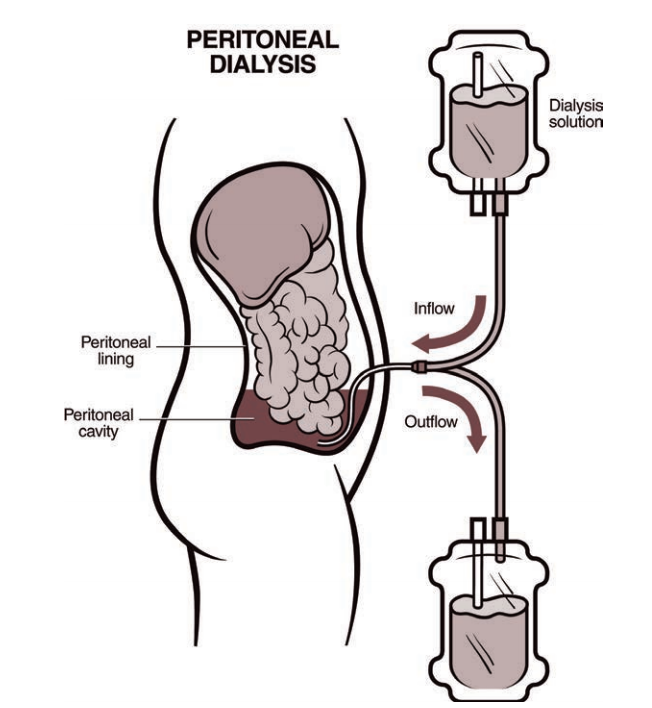
A client is receiving continuous ambulatory peritoneal dialysis since the arteriovenous (AV) graft in the right arm is no longer available for use for hemodialysis. The client has lost weight, has increasing peripheral edema, and has a serum albumin level of 1.5 g/dL (15 g/L). Which intervention is the priority for the nurse to implement?
Serum Albumin Reference Range: 3.5 to 5.5 g/dL (35 to 55 g/L)
A. Recommend the use of support stockings to enhance venous return
Support stockings may help with peripheral edema, but they are not the priority intervention for this client. The client's low serum albumin level indicates malnutrition and increased risk of infection and poor wound healing.
B. Ensure the client receives frequent small meals containing complete proteins
This is the correct answer because the client needs adequate protein intake to maintain serum albumin levels and prevent further complications. Complete proteins contain all nine essential amino acids that the body cannot synthesize and are found in animal sources such as meat, eggs, and dairy products.
C. Evaluate patency of the AV graft for resumption of hemodialysis
Evaluating patency of the AV graft is not the priority intervention for this client because the client is receiving peritoneal dialysis, not hemodialysis. The AV graft may be used in the future if peritoneal dialysis fails, but it is not an immediate concern.
D. Instruct the client to continue to follow the prescribed rigid fluid restriction amounts
Instructing the client to follow fluid restriction amounts is important for peritoneal dialysis patients, but it is not the priority intervention for this client. The client's low serum albumin level indicates that fluid restriction alone is not sufficient to manage fluid balance and prevent edema.
Full Explanation
Choice A reason: Support stockings may help with peripheral edema, but they are not the priority intervention for this client. The client's low serum albumin level indicates malnutrition and increased risk of infection and poor wound healing.
Choice C reason: Evaluating patency of the AV graft is not the priority intervention for this client because the client is receiving peritoneal dialysis, not hemodialysis. The AV graft may be used in the future if peritoneal dialysis fails, but it is not an immediate concern.
Choice D reason: Instructing the client to follow fluid restriction amounts is important for peritoneal dialysis patients, but it is not the priority intervention for this client. The client's low serum albumin level indicates that fluid restriction alone is not sufficient to manage fluid balance and prevent edema.
Text 1:
The nurse is providing lifestyle change education for a client to slow the progression of coronary artery disease. Which statement(s) made by the client should the nurse recognize as needing additional education? (Select all that apply.)
A. Consume foods with saturated fats.
Consuming foods with saturated fats can increase the level of low-density lipoprotein (LDL) cholesterol in the blood, which can contribute to plaque formation and narrowing of the coronary arteries.
B. Walk 30 minutes per day.
Walking 30 minutes per day can help lower blood pressure, improve blood circulation, and reduce the risk of heart attack and stroke.
C. Use a salt substitute.
Using a salt substitute can help lower sodium intake, which can reduce fluid retention and lower blood pressure.
D. Keep a food diary.
Keeping a food diary can help the client monitor their calorie intake, portion size, and nutritional balance.
E. Eat more canned vegetables.
Eating more canned vegetables can increase sodium intake, which can worsen fluid retention and blood pressure. Fresh or frozen vegetables are preferable.
F. Include oatmeal for breakfast.
Including oatmeal for breakfast can provide soluble fiber, which can lower LDL cholesterol and prevent plaque formation in the coronary arteries.
Full Explanation
Choice A reason: Consuming foods with saturated fats can increase the level of low-density lipoprotein (LDL) cholesterol in the blood, which can contribute to plaque formation and narrowing of the coronary arteries.
Choice B reason: Walking 30 minutes per day can help lower blood pressure, improve blood circulation, and reduce the risk of heart attack and stroke.
Choice C reason: Using a salt substitute can help lower sodium intake, which can reduce fluid retention and lower blood pressure.
Choice D reason: Keeping a food diary can help the client monitor their calorie intake, portion size, and nutritional balance.
Choice E reason: Eating more canned vegetables can increase sodium intake, which can worsen fluid retention and blood pressure. Fresh or frozen vegetables are preferable.
Choice F reason: Including oatmeal for breakfast can provide soluble fiber, which can lower LDL cholesterol and prevent plaque formation in the coronary arteries.
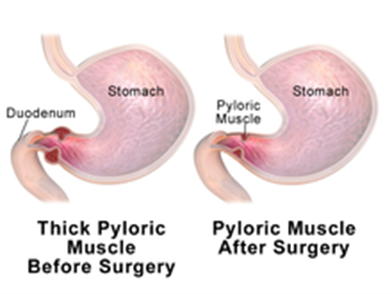
A 6-week-old infant with poor weight gain is scheduled for a pyloromyotomy. Which pre-operative nursing action has the highest priority?
A. Mark an outline of the "olive-shaped" mass in the right epigastric area.
Marking an outline of the "olive-shaped" mass in the right epigastric area is not a priority nursing action. The mass is caused by hypertrophy of the pyloric sphincter, which obstructs gastric emptying and causes projectile vomiting. The mass may not be palpable in all cases.
B. Maintain a continuous infusion of IV fluids per prescription.
This is the correct answer because maintaining a continuous infusion of IV fluids per prescription is essential to prevent dehydration and electrolyte imbalance in the infant. The infant may have significant fluid loss due to vomiting and poor intake.
C. Monitor amount of intake and infant's response to feedings.
Monitoring amount of intake and infant's response to feedings is important, but not the highest priority. The infant may have difficulty feeding due to nausea, vomiting, and abdominal pain.
D. Instruct parents regarding care of the incisional area.
Instructing parents regarding care of the incisional area is a post-operative nursing action, not a pre-operative one. The parents will need to learn how to keep the incision clean and dry, monitor for signs of infection, and administer pain medication as prescribed.
Full Explanation
Choice A reason: Marking an outline of the "olive-shaped" mass in the right epigastric area is not a priority nursing action. The mass is caused by hypertrophy of the pyloric sphincter, which obstructs gastric emptying and causes projectile vomiting. The mass may not be palpable in all cases.
Choice C reason: Monitoring amount of intake and infant's response to feedings is important, but not the highest priority. The infant may have difficulty feeding due to nausea, vomiting, and abdominal pain.
Choice D reason: Instructing parents regarding care of the incisional area is a post-operative nursing action, not a pre-operative one. The parents will need to learn how to keep the incision clean and dry, monitor for signs of infection, and administer pain medication as prescribed.