Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
Which infant would be more likely to have Rh incompatibility?
A. Infant of an Rh-negative mother and a father who is Rh-positive and homozygous for the Rh factor.
Infant of an Rh-negative mother and a father who is Rh-positive and homozygous for the Rh factor. Rh incompatibility occurs when a woman is Rh-negative and her baby is Rh-positive. This can cause hemolytic disease of the neonate (HDN), a condition where the mother’s antibodies destroy the baby’s red blood cells.
B. Infant who is Rh negative and whose mother is Rh negative.
This is wrong because if both the mother and the baby are Rh-negative, there is no risk of Rh incompatibility.
C. Infant of an Rh-negative mother and a father who is Rh-positive and heterozygous for the Rh factor.
This is wrong because if the father is heterozygous for the Rh factor, there is a 50% chance that the baby will be Rh-negative and not affected by Rh incompatibility.
D. Infant who is Rh positive and whose mother is Rh positive.
Thisis wrong because if both the mother and the baby are Rh-positive, there is no risk of Rh incompatibility.
This question is an excerpt from Nurse Dive's nursing test bank - OB Pediatric Cumulative Exam Test 4 V 1 2023 Proctored Exam. Take the full exam now
Full Explanation
choice A.
Infant of an Rh-negative mother and a father who is Rh-positive and homozygous for the Rh factor.
Rh incompatibility occurs when a woman is Rh-negative and her baby is Rh-positive. This can cause hemolytic disease of the neonate (HDN), a condition where the mother’s antibodies destroy the baby’s red blood cells.
Choice B is wrong because if both the mother and the baby are Rh-negative, there is no risk of Rh incompatibility.
Choice C is wrong because if the father is heterozygous for the Rh factor, there is a 50% chance that the baby will be Rh-negative and not affected by Rh incompatibility.
Choice D is wrong because if both the mother and the baby are Rh-positive, there is no risk of Rh incompatibility.
Similar Questions
Human immunodeficiency virus (HIV) may be perinatally transmitted:
A. Only in the third trimester from the maternal circulation.
This is wrong because HIV can be transmitted at any stage of pregnancy, not only in the third trimester.
B. By a needlestick injury at birth from unsterile instruments.
This is wrong because needlestick injury is not a common mode of perinatal transmission of HIV. It is more likely to occur among healthcare workers who are exposed to contaminated needles or sharp objects.
C. Only through the ingestion of amniotic fluid.
This is wrong because HIV can also be transmitted through the ingestion of amniotic fluid, but it is not the only way. Amniotic fluid is the fluid that surrounds and protects the baby in the womb.
D. Through the ingestion of breast milk from an infected mother.
Perinatal transmission of HIV is when HIV is passed from a woman with HIV to her child during pregnancy, childbirth, or breastfeeding. Breast milk from an infected mother can contain HIV and infect the baby.
Full Explanation
The correct answer is choice D. Perinatal transmission of HIV is when HIV is passed from a woman with HIV to her child during pregnancy, childbirth, or breastfeeding.
Breast milk from an infected mother can contain HIV and infect the baby.
Choice A is wrong because HIV can be transmitted at any stage of pregnancy, not only in the third trimester.
Choice B is wrong because needlestick injury is not a common mode of perinatal transmission of HIV. It is more likely to occur among health care workers who are exposed to contaminated needles or sharp objects.
Choice C is wrong because HIV can also be transmitted through the ingestion of amniotic fluid, but it is not the only way. Amniotic fluid is the fluid that surrounds and protects the baby in the womb.
A premature infant with respiratory distress syndrome receives artificial surfactant. How would the nurse explain surfactant therapy to the parents?
A. “Surfactant improves the ability of your baby’s lungs to exchange oxygen and carbon dioxide.”.
Surfactant improves the ability of your baby’s lungs to exchange oxygen and carbon dioxide. Surfactant is a substance that coats the inner surface of the alveoli, the tiny air sacs in the lungs. It reduces the surface tension of the alveoli and prevents them from collapsing during exhalation. Premature infants often lack enough surfactant, which leads to respiratory distress syndrome (RDS). Artificial surfactant is given to these infants to help them breathe more easily.
B. “The drug keeps your baby from requiring too much sedation.”.
This is wrong because surfactant has nothing to do with sedation. Sedation is a state of reduced consciousness induced by drugs. Surfactant does not affect the level of consciousness of the infant.
C. “Surfactant is used to reduce episodes of periodic apnea.”.
This is wrong because surfactant is not used to reduce episodes of periodic apnea. Periodic apnea is a condition where the infant stops breathing for a short time, usually due to immature brainstem function. Surfactant does not affect the brainstem or the control of breathing.
D. “Your baby needs this medication to fight a possible respiratory tract infection.”.
This is wrong because surfactant is not used to fight a possible respiratory tract infection. Surfactant does not have any antibacterial or antiviral properties. Surfactant is used to treat RDS, which is caused by a lack of surfactant, not by an infection.
Full Explanation
choice A. Surfactant improves the ability of your baby’s lungs to exchange oxygen and carbon dioxide.
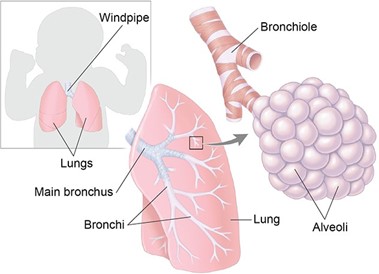
Surfactant is a substance that coats the inner surface of the alveoli, the tiny air sacs in the lungs.
It reduces the surface tension of the alveoli and prevents them from collapsing during exhalation.
Premature infants often lack enough surfactant, which leads to respiratory distress syndrome (RDS).
Artificial surfactant is given to these infants to help them breathe more easily. Choice B is wrong because surfactant has nothing to do with sedation.
Sedation is a state of reduced consciousness induced by drugs. Surfactant does not affect the level of consciousness of the infant.
Choice C is wrong because surfactant is not used to reduce episodes of periodic apnea.
Periodic apnea is a condition where the infant stops breathing for a short time, usually due to immature brainstem function.
Surfactant does not affect the brainstem or the control of breathing.
Choice D is wrong because surfactant is not used to fight a possible respiratory tract infection. Surfactant does not have any antibacterial or antiviral properties.
Surfactant is used to treat RDS, which is caused by a lack of surfactant, not by an infection.
A macrosomic infant is born after a difficult forceps-assisted delivery.
After stabilization, the infant is weighed, and the birth weight is 4550 g (9 lbs, 6 ounces). The nurse’s most appropriate action is to:
A. Leave the infant in the room with the mother.
This is wrong because leaving the infant in the room with the mother without monitoring the blood glucose levels may miss signs of hypoglycemia and delay treatment.
B. Take the infant immediately to the nursery.
This is wrong because taking the infant immediately to the nursery may separate the infant from the mother and interfere with breastfeeding, which can help prevent hypoglycemia.
C. Perform a gestational age assessment to determine whether the infant is large for gestational age.
Thisis wrong because performing a gestational age assessment to determine whether the infant is large for gestational age is not urgent and does not address the risk of hypoglycemia. Normal ranges for blood glucose levels in term infants are 2.6 mmol/L or higher at any time. A blood glucose level of 2.5 mmol/L or less is considered hypoglycemic.
D. Monitor blood glucose levels frequently and observe closely for signs of hypoglycemia.
This is because a macrosomic infant (a newborn who’s much larger than average) is at risk of developing low blood sugar levels after birth, especially if the mother has diabetes. Hypoglycemia can cause neurological damage in the newborn, so it is important to detect and treat it promptly.
Full Explanation
choice D. Monitor blood glucose levels frequently and observe closely for signs of hypoglycemia. This is because a macrosomic infant (a newborn who’s much larger than average) is at risk of developing low blood sugar levels after birth, especially if the mother has diabetes. Hypoglycemia can cause neurological damage in the newborn, so it is important to detect and treat it promptly.
Choice A is wrong because leaving the infant in the room with the mother without monitoring the blood glucose levels may miss signs of hypoglycemia and delay treatment.
Choice B is wrong because taking the infant immediately to the nursery may separate the infant from the mother and interfere with breastfeeding, which can help prevent hypoglycemia.
Choice C is wrong because performing a gestational age assessment to determine whether the infant is large for gestational age is not urgent and does not address the risk of hypoglycemia.
Normal ranges for blood glucose levels in term infants are 2.6 mmol/L or higher at any time. A blood glucose level of 2.5 mmol/L or less is considered hypoglycemic.