Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
Which nursing intervention has priority as a patient diagnosed with anorexia nervosa begins to gain weight after initiating therapy?
Select one:
A. Assess for depression and anxiety every shift
B. Communicate empathy for the patient's feelings to increase rapport
C. Help the patient balance energy expenditure and caloric intake.
D. Observe for adverse effects of refeeding.
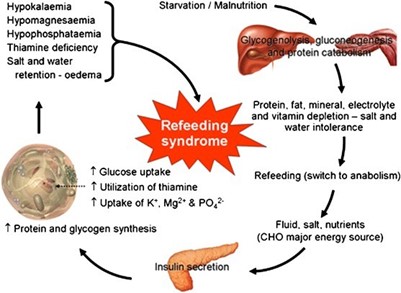
Refeeding syndrome is a potentially life-threatening condition that can occur when a person with anorexia nervosa begins to eat again after a period of starvation. It is important for the nurse to closely monitor the patient for signs of refeeding syndrome, such as electrolyte imbalances and fluid overload, as the patient begins to gain weight.
This question is an excerpt from Nurse Dive's nursing test bank - Mental Health - Proctored Exam 2. Take the full exam now
Full Explanation
Refeeding syndrome is a potentially life-threatening condition that can occur when a person with anorexia nervosa begins to eat again after a period of starvation. It is important for the nurse to closely monitor the patient for signs of refeeding syndrome, such as electrolyte imbalances and fluid overload, as the patient begins to gain weight.
Similar Questions
Which individual with a mental illness may need emergency involuntary hospitalization for mental illness?
The individual who:
Select one:
A. want to hurt a neighbor due to command hallucinations.
Involuntary hospitalization for mental illness is typically reserved for situations where an individual poses an immediate danger to themselves or others due to a severe mental illness. In option A, the individual is experiencing command hallucinations, which are often a symptom of a severe mental illness such as schizophrenia. The fact that they want to hurt their neighbor is a clear indication that they pose a danger to others and require emergency intervention.
B. reports hearing angels playing harps during storms.
Option B may indicate a mental illness such as schizophrenia or bipolar disorder, but it does not necessarily pose an immediate danger to the individual or others.
C. resumes using heroin every day while still taking treatment with methadone.
Option C may indicate a relapse in addiction, but again, it does not necessarily pose an immediate danger to the individual or others.
D. does not show up for a very important appointment in the Mental health clinic
Option D may indicate a need for follow-up and intervention, but it does not indicate an immediate danger to the individual or others.
Full Explanation
Involuntary hospitalization for mental illness is typically reserved for situations where an individual poses an immediate danger to themselves or others due to a severe mental illness. In option A, the individual is experiencing command hallucinations, which are often a symptom of a severe mental illness such as schizophrenia. The fact that they want to hurt their neighbor is a clear indication that they pose a danger to others and require emergency intervention.
Option B may indicate a mental illness such as schizophrenia or bipolar disorder, but it does not necessarily pose an immediate danger to the individual or others.
Option C may indicate a relapse in addiction, but again, it does not necessarily pose an immediate danger to the individual or others.
Option D may indicate a need for follow-up and intervention, but it does not indicate an immediate danger to the individual or others.
A young female client is admitted to the emergency room because she was raped that evening by her date.
How should the registered nurse record the client's chief complaint in the medical record?
A. Gent clams that she was forced to participate in sexual intercourse by a friend
Option a uses colloquial language and may not accurately convey the severity and trauma of the situation.
B. Client States “my date raped me tonight."
This statement clearly and accurately conveys the client's complaint of being raped by her date. It's important for healthcare providers to use appropriate language when documenting sensitive situations like sexual assault to ensure clear communication among the healthcare team and accurate documentation for legal and forensic purposes.
C. Client has been sexually assaulted last night at 10 pm
Option c uses vague language that does not clearly state the nature of the incident.
D. Client reported that she had sexual relations against her Will and she feels very bad
Option d uses subjective language that may not be helpful for accurately documenting the client's complaint.
Full Explanation
This statement clearly and accurately conveys the client's complaint of being raped by her date.
Option a uses colloquial language and may not accurately convey the severity and trauma of the situation.
Option c uses vague language that does not clearly state the nature of the incident.
Option d uses subjective language that may not be helpful for accurately documenting the client's complaint.
It's important for healthcare providers to use appropriate language when documenting sensitive situations like sexual assault to ensure clear communication among the healthcare team and accurate documentation for legal and forensic purposes.
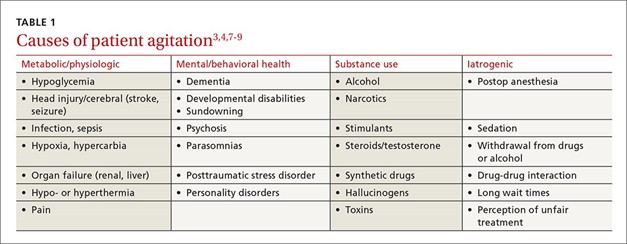
A client is agitated and pacing in the hall near the nurses' station and swearing loudly. What response is the best for the registered nurse to provide?
Select one:
A. Others are being distracted; Please, quiet down and go to your room.
Option a ("Others are being distracted; Please, quiet down and go to your room") is dismissive of the client's feelings and may further escalate the situation.
B. You seem pretty upset. Tell me about it
This response acknowledges the client's distress and opens the opportunity for the client to express their feelings and concerns. It also demonstrates empathy and a willingness to listen, which can help deescalate the situation and build trust between the nurse and client.
C. Please go to your room to get control of yourself.
Option c ("Please go to your room to get control of yourself") is directive and may be perceived as confrontational, potentially increasing the client's agitation.
D. What’s going on? Be quiet.
Option d ("What's going on? Be quiet") is insensitive and dismissive of the client's distress and may further agitate the client.
Full Explanation
This response acknowledges the client's distress and opens the opportunity for the client to express their feelings and concerns. It also demonstrates empathy and a willingness to listen, which can help deescalate the situation and build trust between the nurse and client.
Option a ("Others are being distracted; Please, quiet down and go to your room") is dismissive of the client's feelings and may further escalate the situation.
Option c ("Please go to your room to get control of yourself") is directive and may be perceived as confrontational, potentially increasing the client's agitation.
Option d ("What's going on? Be quiet") is insensitive and dismissive of the client's distress and may further agitate the client.