Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
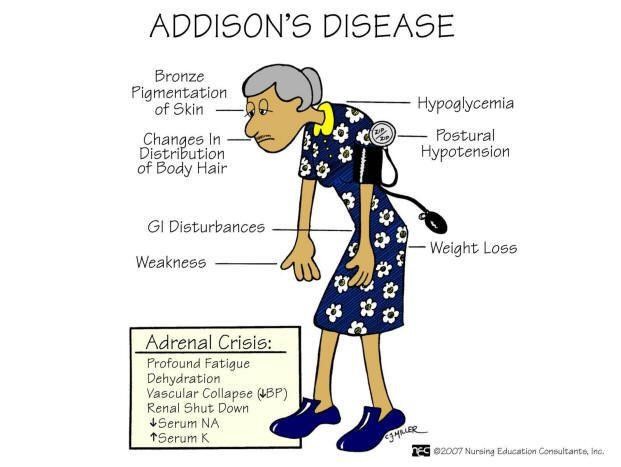
Which of the following would be the most appropriate nursing diagnosis for a client admitted with Addison's disease?
A. Impaired skin integrity
Reason: Impaired skin integrity is not the most appropriate nursing diagnosis for a client with Addison's disease, as it does not reflect the main problem of adrenal insufficiency and cortisol deficiency.
B. Fluid volume overload
Reason: Fluid volume overload is not the most appropriate nursing diagnosis for a client with Addison's disease, as it does not reflect the main problem of adrenal insufficiency and aldosterone deficiency.
C. Imbalanced nutrition: more than body requirements
Reason: Imbalanced nutrition: more than body requirements is not the most appropriate nursing diagnosis for a client with Addison's disease, as it does not reflect the main problem of adrenal insufficiency and weight loss.
D. Risk for injury
Reason: Risk for injury is the most appropriate nursing diagnosis for a client with Addison's disease, as it reflects the main problem of adrenal insufficiency and hypotension, which can cause falls, fainting, or shock.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Proctored Exam 3. Take the full exam now
Full Explanation
Choice A Reason: Impaired skin integrity is not the most appropriate nursing diagnosis for a client with Addison's disease, as it does not reflect the main problem of adrenal insufficiency and cortisol deficiency.
Choice B Reason: Fluid volume overload is not the most appropriate nursing diagnosis for a client with Addison's disease, as it does not reflect the main problem of adrenal insufficiency and aldosterone deficiency.
Choice C Reason: Imbalanced nutrition: more than body requirements is not the most appropriate nursing diagnosis for a client with Addison's disease, as it does not reflect the main problem of adrenal insufficiency and weight loss.
Choice D Reason: Risk for injury is the most appropriate nursing diagnosis for a client with Addison's disease, as it reflects the main problem of adrenal insufficiency and hypotension, which can cause falls, fainting, or shock.
Similar Questions
A home health nurse reinforces instructions to a client who is taking allopurinol for the treatment of gout. The nurse provides which client instructions?
A. Place an ice pack on the lips if they swell.
Reason: Placing an ice pack on the lips if they swell is not an appropriate instruction for a client who is taking allopurinol, as it may indicate an allergic reaction or angioedema, which requires immediate medical attention.
B. Use an over-the-counter (OTC) antihistamine lotion if a rash develops.
Reason: Using an OTC antihistamine lotion if a rash develops is not an appropriate instruction for a client who is taking allopurinol, as it may indicate a serious skin reaction such as Stevens-Johnson syndrome or toxic epidermal necrolysis, which requires immediate medical attention.
C. Drink at least 8 glasses of fluid every day.
Reason: Drinking at least 8 glasses of fluid every day is an appropriate instruction for a client who is taking allopurinol, as it helps to prevent kidney stones and flush out uric acid from the body.
D. Take the medication on an empty stomach 2 hours before meals.
Reason: Taking the medication on an empty stomach 2 hours before meals is not an appropriate instruction for a client who is taking allopurinol, as it may cause stomach upset or nausea. The medication should be taken after meals with plenty of water.
Full Explanation
Choice A Reason: Placing an ice pack on the lips if they swell is not an appropriate instruction for a client who is taking allopurinol, as it may indicate an allergic reaction or angioedema, which requires immediate medical attention.
Choice B Reason: Using an OTC antihistamine lotion if a rash develops is not an appropriate instruction for a client who is taking allopurinol, as it may indicate a serious skin reaction such as Stevens-Johnson syndrome or toxic epidermal necrolysis, which requires immediate medical attention.
Choice C Reason: Drinking at least 8 glasses of fluid every day is an appropriate instruction for a client who is taking allopurinol, as it helps to prevent kidney stones and flush out uric acid from the body.
Choice D Reason: Taking the medication on an empty stomach 2 hours before meals is not an appropriate instruction for a client who is taking allopurinol, as it may cause stomach upset or nausea. The medication should be taken after meals with plenty of water.
A client with a fracture of the left arm that has been set in a cast complains of severe, diffuse pain that is unrelieved by pain medication. The nurse notes that the pulse distal to the site of injury has weakened and that the tissue is pale. Which of the following nursing actions should the nurse perform first?
A. Contact the health care provider.
Reason: Contacting the health care provider is the first nursing action that the nurse should perform, as it indicates that the client may have compartment syndrome, which is a medical emergency that requires immediate intervention to prevent tissue necrosis and nerve damage.
B. Administer PRN pain medication.
Reason: Administering PRN pain medication is not the first nursing action that the nurse should perform, as it may not relieve the pain and may mask the symptoms of compartment syndrome.
C. Document the findings.
Reason: Documenting the findings is not the first nursing action that the nurse should perform, as it may delay the treatment and worsen the outcome of compartment syndrome.
D. Elevate the extremity.
Reason: Elevating the extremity is not the first nursing action that the nurse should perform, as it may decrease blood flow and increase tissue ischemia in compartment syndrome.
Full Explanation
Choice A Reason: Contacting the health care provider is the first nursing action that the nurse should perform, as it indicates that the client may have compartment syndrome, which is a medical emergency that requires immediate intervention to prevent tissue necrosis and nerve damage.
Choice B Reason: Administering PRN pain medication is not the first nursing action that the nurse should perform, as it may not relieve the pain and may mask the symptoms of compartment syndrome.
Choice C Reason: Documenting the findings is not the first nursing action that the nurse should perform, as it may delay the treatment and worsen the outcome of compartment syndrome.
Choice D Reason: Elevating the extremity is not the first nursing action that the nurse should perform, as it may decrease blood flow and increase tissue ischemia in compartment syndrome.
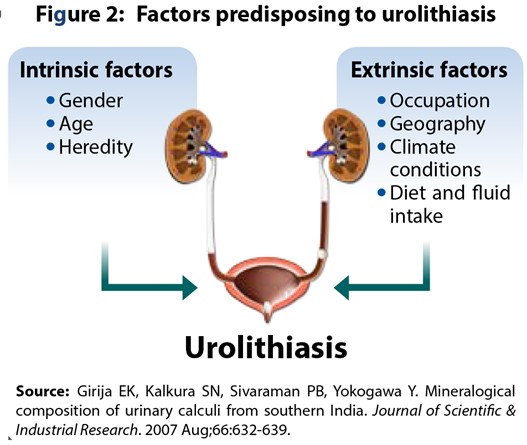
A nurse is contributing to the plan of care for a client who has urolithiasis. Which of the following interventions should the nurse include in the plan?
A. Tell the client to expect a decrease in urine output.
Reason: Telling the client to expect a decrease in urine output is not an appropriate intervention for a client who has urolithiasis, as it may indicate dehydration, obstruction, or infection.
B. Encourage the client to drink 3 L of fluids per day.
Reason: Encouraging the client to drink 3 L of fluids per day is an appropriate intervention for a client who has urolithiasis, as it helps to flush out stones, prevent new stone formation, and reduce urinary concentration.
C. Provide the client with a high protein diet.
Reason: Providing the client with a high protein diet is not an appropriate intervention for a client who has urolithiasis, as it may increase uric acid and calcium excretion and promote stone formation.
D. Maintain the client on bed rest.
Reason: Maintaining the client on bed rest is not an appropriate intervention for a client who has urolithiasis, as it may decrease renal perfusion and increase urinary stasis.
Full Explanation
Choice A Reason: Telling the client to expect a decrease in urine output is not an appropriate intervention for a client who has urolithiasis, as it may indicate dehydration, obstruction, or infection.
Choice B Reason: Encouraging the client to drink 3 L of fluids per day is an appropriate intervention for a client who has urolithiasis, as it helps to flush out stones, prevent new stone formation, and reduce urinary concentration.
Choice C Reason: Providing the client with a high protein diet is not an appropriate intervention for a client who has urolithiasis, as it may increase uric acid and calcium excretion and promote stone formation.
Choice D Reason: Maintaining the client on bed rest is not an appropriate intervention for a client who has urolithiasis, as it may decrease renal perfusion and increase urinary stasis.