Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A client presents to the clinic with complaints of otalgia and muffled sounds. The client is diagnosed with external otitis. Which of the following will the nurse not include in client teaching?
A. Report itching if it becomes bothersome
Reason: Reporting itching if it becomes bothersome is part of client teaching, as it may indicate inflammation or infection of the ear canal. External otitis is also known as swimmer's ear, as it can be caused by water trapped in the ear after swimming or bathing.
B. Use earplugs when swimming
Reason: Using earplugs when swimming is part of client teaching, as it can prevent water from entering and irritating the ear canal. External otitis can be prevented by keeping the ear dry and avoiding trauma or foreign objects.
C. Insert a cotton-tip applicator to remove excess wax
Reason: This is the correct choice. Inserting a cotton-tip applicator to remove excess wax is not part of client teaching, as it can damage or scratch the ear canal and increase the risk of infection. Wax helps protect and lubricate the ear canal and should not be removed unless it causes hearing impairment or discomfort.
D. Use a hairdryer set to low, 6 inches away from ear
Reason: Using a hairdryer set to low, 6 inches away from ear is part of client teaching, as it can help dry the ear canal after swimming or bathing. External otitis can be treated by applying warm compresses, using topical antibiotics or antifungals, and taking pain relievers or anti-inflammatory drugs.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Proctored Exam 4. Take the full exam now
Full Explanation
Choice A Reason: Reporting itching if it becomes bothersome is part of client teaching, as it may indicate inflammation or infection of the ear canal. External otitis is also known as swimmer's ear, as it can be caused by water trapped in the ear after swimming or bathing.
Choice B Reason: Using earplugs when swimming is part of client teaching, as it can prevent water from entering and irritating the ear canal. External otitis can be prevented by keeping the ear dry and avoiding trauma or foreign objects.
Choice C Reason: This is the correct choice. Inserting a cotton-tip applicator to remove excess wax is not part of client teaching, as it can damage or scratch the ear canal and increase the risk of infection. Wax helps protect and lubricate the ear canal and should not be removed unless it causes hearing impairment or discomfort.
Choice D Reason: Using a hairdryer set to low, 6 inches away from ear is part of client teaching, as it can help dry the ear canal after swimming or bathing. External otitis can be treated by applying warm compresses, using topical antibiotics or antifungals, and taking pain relievers or anti-inflammatory drugs.
Similar Questions
A client arrives with an upper respiratory infection and complains of otalgia, malaise, and nasal drainage. The client's temperature is 100.7 F. Which of the following will the nurse anticipate providing to the client?
A. Education about mastoidectomy
reason: This is incorrect because education about mastoidectomy is not relevant for a client with an upper respiratory infection. Mastoidectomy is a surgical procedure that removes part or all of the mastoid bone behind the ear, which can become infected or inflamed due to chronic or recurrent middle ear infections. The nurse should assess the client's ear for signs of mastoiditis, such as swelling, tenderness, or redness behind the ear, but mastoidectomy is not a common or first-line treatment for upper respiratory infection.
B. A referral for a hearing test
reason: This is incorrect because a referral for a hearing test is not necessary for a client with an upper respiratory infection. Hearing test is a diagnostic tool that measures how well a person can hear different sounds at different frequencies and intensities. The nurse should ask the client about any changes in hearing or tinnitus, which are possible complications of upper respiratory infection, but a hearing test is not a routine or urgent intervention for this condition.
C. Education on administration of oral antibiotics
reason: This is correct because education on the administration of oral antibiotics can help treat an upper respiratory infection. Antibiotics are drugs that kill or inhibit bacteria that cause infections. Upper respiratory infections can be caused by various pathogens, such as viruses, bacteria, or fungi, but bacterial infections are more likely to cause fever, otalgia, or purulent nasal drainage. The nurse should instruct the client on how to take antibiotics as prescribed, such as dosage, frequency, duration, side effects, and interactions.
D. A prescription for an antifungal cream
reason: This is incorrect because a prescription for an antifungal cream is not appropriate for a client
Full Explanation
Choice A reason: This is incorrect because education about mastoidectomy is not relevant for a client with an upper respiratory infection. Mastoidectomy is a surgical procedure that removes part or all of the mastoid bone behind the ear, which can become infected or inflamed due to chronic or recurrent middle ear infections. The nurse should assess the client's ear for signs of mastoiditis, such as swelling, tenderness, or redness behind the ear, but mastoidectomy is not a common or first-line treatment for upper respiratory infection.
Choice B reason: This is incorrect because a referral for a hearing test is not necessary for a client with an upper respiratory infection. Hearing test is a diagnostic tool that measures how well a person can hear different sounds at different frequencies and intensities. The nurse should ask the client about any changes in hearing or tinnitus, which are possible complications of upper respiratory infection, but a hearing test is not a routine or urgent intervention for this condition.
Choice C reason: This is correct because education on the administration of oral antibiotics can help treat an upper respiratory infection. Antibiotics are drugs that kill or inhibit bacteria that cause infections. Upper respiratory infections can be caused by various pathogens, such as viruses, bacteria, or fungi, but bacterial infections are more likely to cause fever, otalgia, or purulent nasal drainage. The nurse should instruct the client on how to take antibiotics as prescribed, such as dosage, frequency, duration, side effects, and interactions.
Choice D reason: This is incorrect because a prescription for an antifungal cream is not appropriate for a client
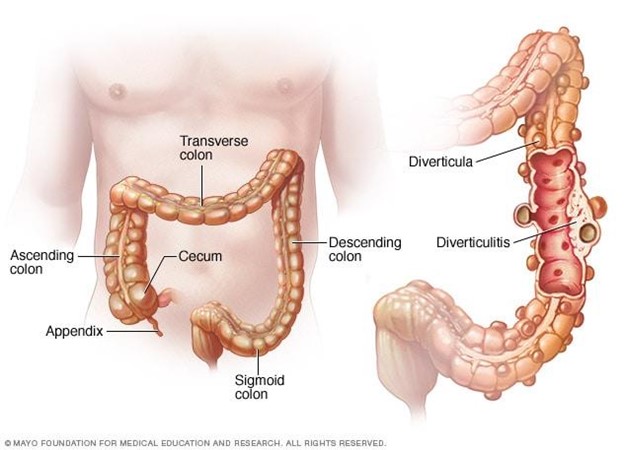
A nurse is creating an education plan for a client who has diverticulosis. The nurse should plan to include which of the following in the client education?
A. Increase protein from red meat
Reason: Increasing protein from red meat is not part of client education, as it can worsen the condition and increase the risk of complications. Red meat is high in fat and low in fiber, which can cause constipation and increase the pressure in the colon. Diverticulosis is a condition where small pouches or sacs form in the wall of the colon due to weak spots or increased pressure.
B. Decrease fluid intake
Reason: Decreasing fluid intake is not part of client education, as it can worsen the condition and increase the risk of complications. Fluid intake should be increased to prevent dehydration and promote bowel movements. Diverticulosis can cause abdominal pain, bloating, cramping, and changes in bowel habits.
C. Incorporate soft foods that are pureed in consistency
Reason: Incorporating soft foods that are pureed in consistency is not part of client education, as it can worsen the condition and increase the risk of complications. Soft foods are low in fiber and can cause constipation and increase the pressure in the colon. Diverticulosis can lead to diverticulitis, which is inflammation or infection of the pouches or sacs.
D. Increase dietary fiber
Reason: This is the correct choice. Increasing dietary fiber is part of client education, as it can improve the condition and prevent complications. Fiber helps soften the stool and reduce the pressure in the colon. Diverticulosis can be managed by eating a high-fiber diet, drinking plenty of fluids, exercising regularly, and avoiding straining or holding stools.
Full Explanation
Choice A Reason: Increasing protein from red meat is not part of client education, as it can worsen the condition and increase the risk of complications. Red meat is high in fat and low in fiber, which can cause constipation and increase the pressure in the colon. Diverticulosis is a condition where small pouches or sacs form in the wall of the colon due to weak spots or increased pressure.
Choice B Reason: Decreasing fluid intake is not part of client education, as it can worsen the condition and increase the risk of complications. Fluid intake should be increased to prevent dehydration and promote bowel movements. Diverticulosis can cause abdominal pain, bloating, cramping, and changes in bowel habits.
Choice C Reason: Incorporating soft foods that are pureed in consistency is not part of client education, as it can worsen the condition and increase the risk of complications. Soft foods are low in fiber and can cause constipation and increase the pressure in the colon. Diverticulosis can lead to diverticulitis, which is inflammation or infection of the pouches or sacs.
Choice D Reason: This is the correct choice. Increasing dietary fiber is part of client education, as it can improve the condition and prevent complications. Fiber helps soften the stool and reduce the pressure in the colon. Diverticulosis can be managed by eating a high-fiber diet, drinking plenty of fluids, exercising regularly, and avoiding straining or holding stools.
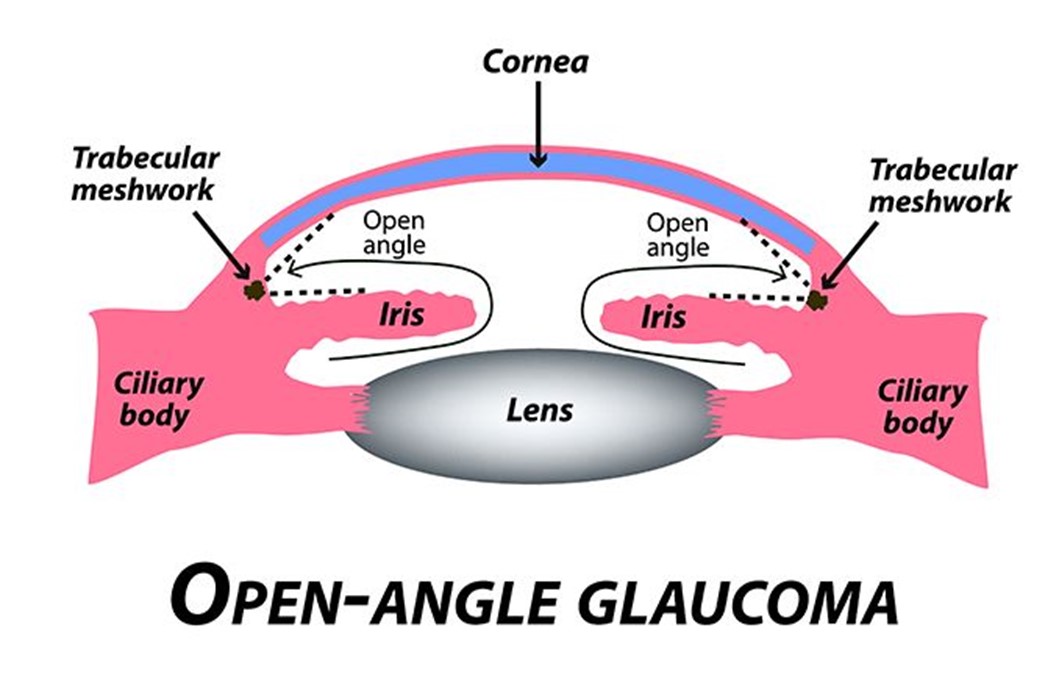
A nurse at an ophthalmology clinic is providing teaching to a client who has open-angle glaucoma and a new treatment regimen of timolol and pilocarpine eye drops. Which of the following instructions should the nurse provide?
A. It is not necessary to remove contact lenses before administering medications
reason: This is incorrect because it is necessary to remove contact lenses before administering medications. Contact lenses can absorb or interfere with the absorption of eye drops and cause irritation or infection. The nurse should instruct the client to remove contact lenses before applying eye drops and wait at least 15 minutes before reinserting them.
B. Administer the medications by touching the tip of the dropper to the sclera of the eye
reason: This is incorrect because administering the medications by touching the tip of the dropper to the sclera of the eye can cause contamination or injury. The sclera is the white part of the eye that covers most of the eyeball. The nurse should instruct the client to avoid touching the tip of the dropper to any part of the eye or eyelid and hold it about 1 cm above the lower eyelid.
C. Administer the medications 5 min apart
reason: This is correct because administering the medications 5 min apart can prevent dilution or washout of one medication by another. Timolol and pilocarpine are two different types of eye drops that are used to treat open-angle glaucoma, which is a condition that causes increased pressure inside the eye and damage to the optic nerve. Timolol is a beta-blocker that reduces the production of fluid in the eye, and pilocarpine is a cholinergic agent that increases the drainage of fluid from the eye. The nurse should instruct the client to apply one drop of each medication in the affected eye(s) and wait at least 5 minutes between each medication.
D. Hold pressure on the conjunctival sac for 2 minutes following the application of eye drops
reason: This is incorrect because holding pressure on the conjunctival sac for 2 min following the application of eye drops can reduce systemic absorption and side effects of eye drops. The conjunctival sac is the space between the lower eyelid and the eyeball. The nurse should instruct the client to gently close their eyes after applying eye drops and press their index finger against the inner corner of their eye for 2 minutes. This can block the tear duct that drains fluid from the eye to the nose and prevent it from entering the bloodstream.
Full Explanation
Choice A reason: This is incorrect because it is necessary to remove contact lenses before administering medications. Contact lenses can absorb or interfere with the absorption of eye drops and cause irritation or infection. The nurse should instruct the client to remove contact lenses before applying eye drops and wait at least 15 minutes before reinserting them.
Choice B reason: This is incorrect because administering the medications by touching the tip of the dropper to the sclera of the eye can cause contamination or injury. The sclera is the white part of the eye that covers most of the eyeball. The nurse should instruct the client to avoid touching the tip of the dropper to any part of the eye or eyelid and hold it about 1 cm above the lower eyelid.
Choice C reason: This is correct because administering the medications 5 min apart can prevent dilution or washout of one medication by another. Timolol and pilocarpine are two different types of eye drops that are used to treat open-angle glaucoma, which is a condition that causes increased pressure inside the eye and damage to the optic nerve. Timolol is a beta-blocker that reduces the production of fluid in the eye, and pilocarpine is a cholinergic agent that increases the drainage of fluid from the eye. The nurse should instruct the client to apply one drop of each medication in the affected eye(s) and wait at least 5 minutes between each medication.
Choice D reason: This is incorrect because holding pressure on the conjunctival sac for 2 min following the application of eye drops can reduce systemic absorption and side effects of eye drops. The conjunctival sac is the space between the lower eyelid and the eyeball. The nurse should instruct the client to gently close their eyes after applying eye drops and press their index finger against the inner corner of their eye for 2 minutes. This can block the tear duct that drains fluid from the eye to the nose and prevent it from entering the bloodstream.